Physical Activity Trajectories Preceding Incident Major Depressive Disorder Diagnosis Using Consumer Wearable Devices in the All of Us Research Program: Case-Control Study
Low physical activity is a known risk factor for major depressive disorder (MDD), but changes in activity before a first clinical diagnosis remain unclear, especially using long-term objective measurements. This study characterized trajectories of we…
Authors: Yuezhou Zhang, Amos Folarin, Hugh Logan Ellis
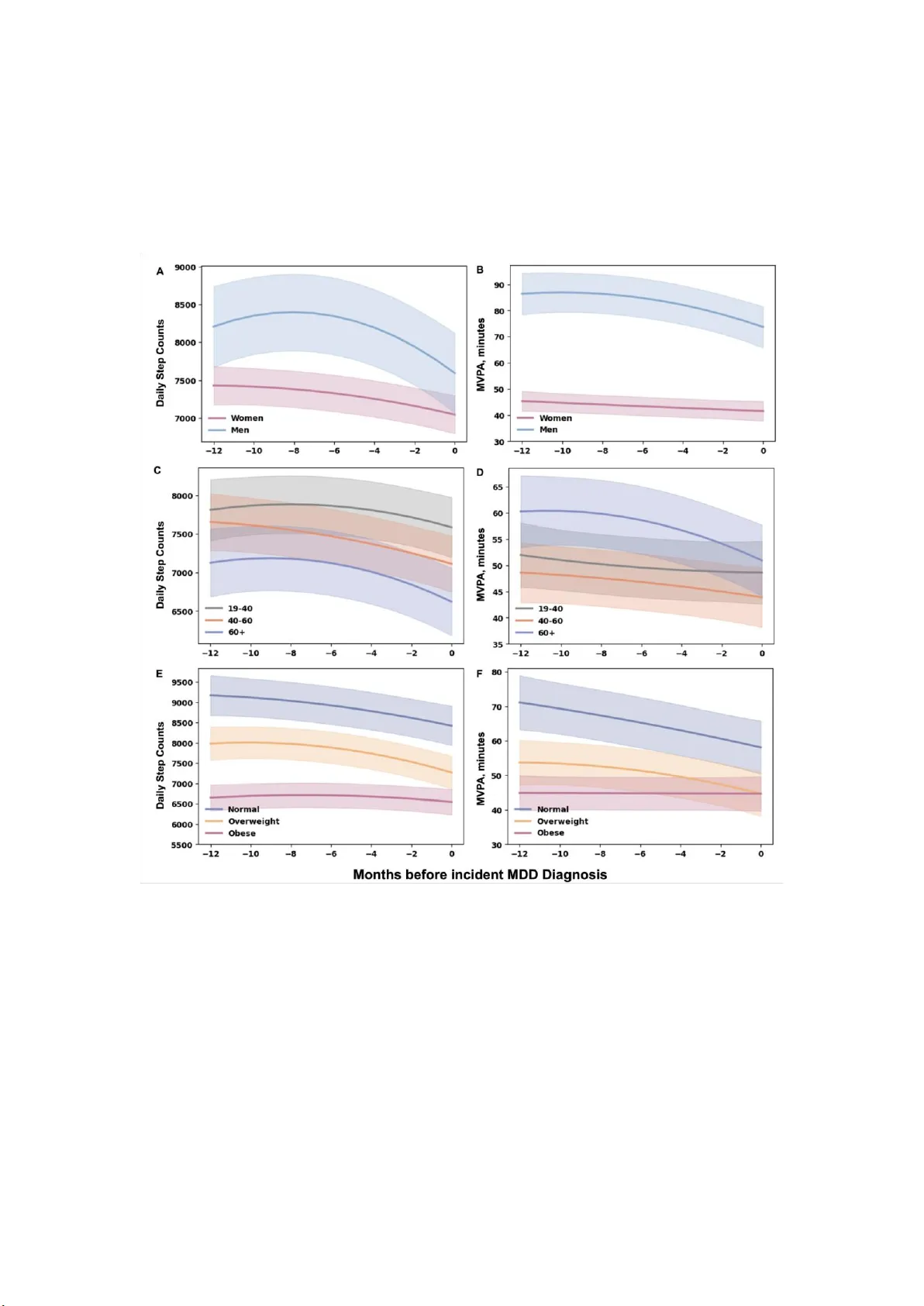
1 Physical Activity T rajectories Pr eceding In cident Major De pr essive D iso rder Diagnosis Using Consu m er W e arable Devices in the All of Us Research Pr ogram: Case-C ontrol Stud y Y uezhou Zhang 1 , PhD; Amos Folarin 1,2,3,4,5 , PhD; Hugh Logan Ellis 1 , MbBChi r; Rongrong Zhong 1,6 , MD; Callum S tewa rt 1 , PhD; Heet Sankesara 1 , B Sc; Hyunju Kim 1 , PhD; S haoxiong Sun 1,7 , PhD; Abhishek Pratap 1,8,9 , PhD; Ri cha rd JB Dobson 1,2,3,4,5 , PhD 1 Department of Biostatisti cs & He alth Infor matics, Insti tute of Psychiatry , Psychology and Neurosc i ence, King's College London, London, U nited Kingdom 2 Institute of Hea lth In forma tics, University C ollege London, London, United Kingdom 3 NIHR Biomedical Researc h Cent re at South London and Maudsley N HS Foundation T rust, London, United Kingdom 4 NIHR Biomedical Researc h Cent re at Unive rsity Coll ege London Hospitals NHS Foundation T rust, London, United K ingdom 5 Hea lth Dat a Resear ch UK, Universit y College London, London, United Kingdom 6 Clini ca l Resear ch Center & Division of Mood Disorders, Shangha i Mental Health Center , Shanghai Jiao T ong University School of Medicine, Shan ghai, China 7 Department of Computer Science, University of Sheffiel d, Sheffield, United Kingdom 8 Boehringer I ngelheim P har maceuticals, Inc., Ridgefield, C T , U nited States 9 University of W a shington, Seattle, W A, United States Correspond ing author: Richard JB Dobson, PhD Department of Biostatisti cs & He alth Infor matics, Insti tute of Psychiatry , Psychology and Neurosc i ence, King's College London, U nited Kingdom Mail addre ss: PO B ox 80, SGDP Centre, I oPPN, De Cr espigny P ar k, Denmar k Hil l London, SE5 8AF , United Kingdom Email: richard.j.dobson@ k cl.a c.uk Phone: 44 20 7848 0473 2 Abstract Backgrou nd: Low physical ac tivity i s a we ll-e stablished risk fa ctor for major depressive disorder ( MDD). However , how physical activity changes in the months preceding a first clinical diagnosis of MDD ha s not b ee n well explored, pa rticular ly when assessed using long- term, objective measures collec t ed in real -world settings. Objective: This study aimed to charac terize traj ec tories of wearable-measure d physical activity during the year prece ding incid ent MDD dia gnosi s. Met hods: W e conducted a retrospective nested case-control study usi ng linked elec tronic health record (EHR) a nd consumer wearable data (Fitbi t) fr om the All of Us Research Program. A dults with at least 6 months of valid F itbit physica l activity data in the 12 months preceding diagnosis were e ligible. In cident MDD cases were identified based on a first rec orded EHR diagnosis and m atche d to MDD-free controls on age, sex, body ma ss index, and time of diagnosis, with up to four controls per case. Daily step cou nts and moderate- to - vigorous physical ac tivity (MVP A) were aggregated into mont hly ave rages. Linear mixed - effects models were used to compare pre-diagnostic physi ca l activity t raje ctories between case s and controls over a re trospective time scale from −12 to 0 months. A mong case s, within-person contrasts were used to identify when physical activity levels first showed statistically signi fica nt deviations rela tive to levels observ ed 12 months before diagnosis. Exploratory a nalyses ex amined whe ther pre-dia gnostic trajectori es differed by sex, age, and body mass index. Results: The analytic c ohort i ncluded 4,104 participants (829 incident MDD cases a nd 3,275 3 matched c ontrols; 81.7% women; media n age 48.4 years). Compar ed with controls, individuals who developed MDD exhibit ed c onsistently lower overall physical activity l eve ls and significant downward trajec tori es in both daily step counts and MVP A dur ing the y ea r preceding diagnosis (global tra j ec tory tests, P < .001 for both out comes) . Among cases, statistically signi fica nt change s in daily step counts emerg e d approximately 4 months before diagnosis, whereas significant c hanges in MVP A e merg ed approximately 5 months before diagnosis. Furthermore, e xploratory analyses suggested heterogeneity in pre- diagnosti c trajec tories across demogr aphic subgr oups, including steeper declines among men, more pronounce d redu ctions in activity intensity at older age s, and pe rsistently lower activity levels with flatter tra j ec tories among indivi duals with obesity . Conclusion s: In this large cohort with linked wearable an d clinica l data, sustained within- person declines in physical activity emerged several mont hs before incide nt MDD diagnosis. These f indings suggest that longit udinal monitoring of physical ac tivity usi ng consumer wearable devices m ay provide clini ca lly relevant early signals to support risk stratification, targeted prevention, and earlier intervention for MDD. Keywords: Ma jor Depressive Disorder; Depression; Physi ca l Ac tivity; W ea rable Devices; Mobile Health ( mHealth); Longitudinal S tudies; Case-Control Studies; Electronic He alth Records 4 Introd uction Major depressive disorder (MDD) is a lea ding ca us e of di sability worldwide [1] and is associate d with substantial adverse out comes, inc luding p remature mortality [ 2], f unctional impairment [3], inc reased medical comorbidity [4], and suicide [5]. G iv en its substantial individual and societal burde n [1], early identification of i ndividuals in the prodromal or initial st age s of MDD is cr itically important, as preventiv e stra tegies [6] a nd early interventions [7] may be most ef fective during this period. Ho wever, sympt om onset fre quently precedes clini ca l recognition and formal diagnosi s in routine clinical se ttings [8, 9], reflec ting prolonged durations of untr ea ted illness in MD D. Low physical activity (P A) ha s been identified as a risk fa ctor f or MDD in prospective cohort studies and meta-ana lyses [10-12]. Longitudinal evidence further suggests that reductions in P A may prec ede worsening depressive symptoms [13], supporting the possibility t hat de clines in P A c an oc cur before the clinical diagnosis of MDD. However , much of the exist ing evidence re lies on self-reported P A, which is subject to recall bias [1 1] , or on accelerometer - based a ss essments conduc ted over short durations or at infrequent follow-up time points [14]. Consequently , cur rent studies provide limit ed insight into the timing and patter n of P A change s pre ce ding a clinical MDD diagnosis, including w hen P A de viate s from a n individual’ s prior a ctivity level and whe th er these changes di ffer across population subgroups. Addressing these qu estions require s longitudinal, objectiv e mea sures of P A collec t ed in real - world settings and reliably linked to clinical diagnostic infor mation, which allow behavioral change to be ch ar acterized prior to diagnosis as illness unfolds in routi ne c are. 5 Advances in sensor technology and the widespread adoption of consumer wearabl e de vices have e nabled p assive, c ontinuous monit oring of r eal-wor ld P A at sca le, with device s su ch a s Fitbi t trackers c apturing daily st ep c ounts and activity intensity—key correlates of functioning and psychomotor activity [15]—ove r extended periods wi th minimal user burden [16, 17] . Recent mobile health studies have de monstr ated ne gative associa tions between wearable- measure d P A and depression severity [18 -20], suggesting that such measures may co mplement sympt om-ba sed assessments by informing risk stratification and prompting ear lier clinical evaluation. N eve rtheless, prior mobile heal th studies have bee n limited by modest sample sizes, relatively short monitoring durations, or the abse nce of li nkage to clinical diagnoses [18], constraining t heir a bility to chara cter ize behavioral chang es in relation to clinical diagnosis timing. Few large-scale datasets int egra te long- t er m wearable data with electronic health records (EHRs) in a manner that e nables ex amination of pre -diagnostic PA tra jectorie s and subgroup heterogeneity . The A ll of Us Researc h Program (AoURP) provides such an integrated resource, c omprisi ng a large, ongoing national cohort in which pa rticipants consent to share EHRs, health surveys, biospecimens, physical measurements, and weara ble data [ 21]. By linking hist orica l and prospec tive Fitbit data with EHR-based diagnoses, this study enables examination of long- term P A tra jectories preceding clinical MDD diagnosis. Here, we aimed to determine whether P A tra jectories diff er be tween indivi dua ls with incide nt MDD and matched c ontrols during t he 12 months preceding diagnosis. A mong individuals who develope d MDD, we fur ther examined when P A begins to deviate from earlier levels and whether th e pa ttern of pre-diagnostic changes varies across population subgroups. 6 Met hods Stud y participants W e used da t a f rom the AoU RP , an ongoing national longit udinal cohor t funded by the US National Institutes of Health [21] , with the long-term goal of enr olling at least 1 million participants. The study design and data collec tion procedures have be en de scribed previously [21, 22]. The pre sent analysis used the controlled tier d ata set, versi on 8 ( C2024Q3R8), including participants e nroll ed be tween May 2017 and October 2023. P articipant de mographics and baseline da t a were collected during the digit al enr ollment. For participa nts who c onsented to share EHR and Fitbit data, their historical (pre -enrollment) EHR data and Fitbit data were made a vailable through their particip ating health care pro vide r organizations and linked Google Fitbit accounts, respectively [ 21-23]. In this data version, 36,614 individuals had linked EHR and Fitbit data available. Ethical Considerations This study invol ved a sec ondary analysis of deidentified data obtained from the AoU RP a nd theref ore did not r equire additional ethics review . Access t o deide ntified data was restricted to authorize d study investigators who completed required All of Us Responsible Conduct of Research tra ining, and all analyses we re conducted within the secure, c loud- based Res earcher W orkbenc h environment. In ac cor dance with t he AoURP Data and Statistics Dissemination Policy , analytic r esults for groups with fewer than 20 participants were not reported to minimi ze the risk of pa rticipant reidentification. 7 For the AoURP , all participants provided informed consent at enrollment and were informed of their right to withdraw from the program at any time. Data privacy a nd conf id entiality wer e protecte d through multiple safeguards, including secu re cloud -ba sed data storage, restricted access to deide ntified data, and m anda tory confidentiality and data us e a greements. Participant compensa tion of US $25 for the collec tion of bi ological spec imens (eg, blood, saliva, or urine) wa s p rovided by the AoU RP in the f orm of ca sh payments, gift cards, or elec troni c vouc hers, as applicable. Fitbit P A Data P A in this study was quantified using daily step c ounts and m oder ate- to -vigorous physical activity (MVP A) , which intuitively capture overall activit y volume [24] a nd activity i ntensity emphasize d in established public health guidelines [ 25], respec tively . Fitbit classifies activity intensity int o devic e-de fined categories using metabolic equi valent of ta sk (MET)–ba sed criter ia, consist ent with intensity frame works widely adopt ed in re search- grade accelerometry [26, 27]. I n this study , da ily MVP A was ca lcula t ed a s the daily sum of de vice-labe l ed “ fairly active” minutes plus twice th e numbe r of “very active” m inutes, consistent with established definitions [8]. T o e nsure data quality , only da ys with at least 10 hours of wear time and daily step counts betwee n 100 and 45,000 w er e considered valid, following prior A oU RP st udies [28-30]. Monthly avera ges of daily step counts and MVP A minutes we re calculated to reduce day - to - day var i ability relate d to missi ngness a nd short-te rm fluct ua tions, consistent with prior AoU RP analyses [28-30]. Months with more than 10 valid days were considered valid and 8 retaine d for analysis [30]. Incident MDD Cases Following definiti ons used in prior AoU RP re search [28, 31], incident MDD cases were defined as par ticipants whos e f irst recorded MDD di agnosis occurred during their Fitbit monitoring period, with no prior MDD diagnosis. Participants were required to be aged 19 year s or older at the time of dia gnosis to ensure th ey were adults (≥18 yea rs) throughout the 1-year pre-dia gnostic observation period. In addition, i ndividuals with any rec orded diagnosis of bipolar disorde r , schizophrenia, or schizoaffe ctive disorde r prior to the diagnosis date were exclude d. T o ensure suf f icient pre-dia gnostic weara bl e data, ca ses were required to h ave at least 6 valid months of Fitbi t P A data within the 12 months pr eceding the diagnosis month. Diagnoses were identifi ed f rom EHR data using standardized concept identifi er s from the Observa tional M edica l Outcomes Partnership (OMOP) com mon data model, whic h harmonize di agnose s across vocabularies including S NOMED, I CD- 9-CM, and ICD-10-CM [32]. The OMOP concept identifier s us ed in this study , along with their c orresponding ICD- 9- CM and ICD-10- CM codes, are provided in Supplementary T a ble 1. Neste d Case-Control D e sign A ne sted ca se-control design [33-35] was used to constru ct the comparison group. Cases a nd controls were matc hed at the diagnosis month (he reafter referre d to as the ma tching month) on age (within 1 year) , sex, and body m ass index (BMI) c a tegory , which were selected a priori given their strong a ssociations wit h both P A and de pression risk. BMI was defined using the measure m ent close st to one year before the mat ching month to minimize potential 9 influence of emer ging MDD on body weight. Eligible controls were selected from the risk set of par ticipants who, at the matching month, were age d 19 years or older , had no recorded MDD diagnosis, had no prior dia gnosis of bipola r disorder , sc hizophrenia, o r schizoaf fective disorder , and met the same Fitbit P A data availability criter ia as cases. For each case, up to four c ontrols were sele cted, a ratio chosen to improv e statistical e fficiency while maintaining matching quality and consistenc y with prior t ra jectory-based nested case-control studies [33, 34]. When more than four eligible controls were availabl e, controls were randomly sampled without replacement within or between cases to avoid repeated use of the same individuals and to simplify the corre l ation structure of longit udinal ana lyses [ 34]. Additional sociodemogra phic factors were not includ ed in matching to avoid over matching and preserve statistical efficiency . Statistical analysis Linear mixed-ef f ec ts models with pa rticipant- specific random interce pts were used to estimate P A traje ctories over time. A retrospective time scale from −12 to 0 months was defined, w ith time 0 corresponding to the diagnosis mont h for case s and the matching month for c ontrols. Models included cas e –control status (coded as 0 for controls and 1 for cases), linear a nd quadr atic time ter ms (time and time²) to allow f or potential non -linear temporal patterns, a nd their int er action terms, as well as matching vari able s. Dif f erences in trajectories betwee n cases and controls we re evaluated using time×ca se and time²×case interaction terms, with a joint W ald test used to evalua te whether overall temporal patterns diff ered by case - control status. Model-de rived margi nal means were used to estimate and c omp ar e monthly trajec tories between cases and c ontrols. Statist ical significa nce of between-gr oup diff ere nces 10 at each month was a ssessed using contrast P values, with P values a djusted for mult iple comparisons using the Benjamini–Hochbe rg p rocedure [36]. Among individuals with i ncide nt MDD, marginal means were estimated for e ac h month, and pairwise c ont ra sts comparing each month with m onth −12 were used to identify whe n P A began to differ relative to the earliest month. T o assess potential heterogeneity in pr e- diagnostic P A trajec tories, exploratory case-only models we re extended to include interactions betwee n time variabl es and subgr oup indicators for sex, a ge, a nd BMI. Results This study included 4,104 participants, compr ising 829 indi viduals with incident MDD a nd 3,275 matched c ontrols. The median age of the overall cohort was 48.4 years (IQR, 36.3–61.3 year s); 81.7% of participants were wom en, a nd 82.5% were White. Cases and controls had simil ar distributions of age, sex, BMI, race , and ethnicity , with all standardize d mean differences (SMDs) below 0.1, indic ating ade quate balance between groups (T able 1). Participant selec tion and cohort construc tion are shown in Figure 1. P A T r ajector i es Preceding In cident MDD Diagnosis The tra jectories of daily st ep c ounts during the 12 months preceding the matc hing month differed significantly between incid ent MDD case s and matched controls (Figure 2A). In mixed-effects models, controls exhibit ed a relatively stabl e tra jectory , whereas cases showed a marked and accelerating dec line as the diagnosis mont h appr oached. Th e se differ enc es were supported by significant linear and quadratic interaction terms (time × case: β = −92.08; 95% CI, −126.14 to −58.02; time² × case: β = −5.47; 95% CI, −8.23 to −2.70), with a significant 11 global test for tra jectory dif ferences (joint W a ld test, P < .001) (T able 2). Model-derived marginal means indicated that daily step counts wer e c onsi stently lower a mong cases than controls at every month exa mined. As early a s 12 months be fore diagnosis, ca s es a veraged 7568 steps (95% CI, 7330–7806) compared with 8360 steps (95% CI, 8240–8480) a mong controls (contrast difference, −792 steps; 95% CI, −1058 to −525; P < .001). This case– control gap wide ned progressively ove r time, reac hing −1 109 steps (95% CI , −1374 to −845; P < .001) in the matching month, when case s ave ra ged 71 40 ste ps (95% CI, 6904 –7376) and controls average d 8249 st eps (95% CI, 8130–8369) (Supplementar y T able 2) . Simi lar pa tterns we re observed for daily MVP A traje ctories (Figure 2B). Compared with controls, ca s es e xhibited consistently lower daily MVP A le vels throughout the pre-dia gnostic period. In mixed -eff e cts models, diverg ence in MVP A tra jectorie s was supported by a significant linear interac tion (time × ca se: β = −0.78; 95% CI, −1.39 to −0.18) and a significant global test for tra j ec tory dif f e rences (joint W a ld test, P < .001) ( T able 2). Model- derived ma rgin a l means showed that at 12 months before di agnosis, c a ses averaged 52.9 minutes of MVP A (95% CI, 49.2–56.7) compared with 60.9 minut es (95% CI, 59.1–62.8) among controls (c ontrast P < .001). This di ff er ence increa sed over time and reached −1 1.35 minutes (95% CI, −15.48 to −7.22; P < .001) in the matching m onth, when c ases averaged 47.3 minutes (95% CI, 43.7–51.0) a nd controls averaged 58.7 minutes (95% CI, 56.8–60.6) (Supplementary T a ble 3). Timing of Within -Pe rson Pre-diagnostic Changes A mon g Incident MDD Case s T o c haracterize the timing of within-person changes in P A pre ceding diagnosis, we conducted 12 case-only marginal contrasts analyses using 12 months be fore diagnosis (time = −12) as the refere nce. Among cases, da ily step counts did not dif fe r signi fica ntly from the reference level until 4 mont hs befor e diagnosis. A t time = −4, step counts were significantly lower th an a t time = −12 (−145 steps; 95% CI, −253 to −37; P = .02). Reductions became larg er a s diagnosis approached, reaching −428 steps in the matching month (95% CI, −531 to −326; P < .001) (Supplementa ry T able 4). In terms of da ily MVP A, levels among ca s es were signifi cantly lower th an the ref erence level by 5 months before dia gnosis (time = −5: −2.48 minutes; 95% CI, −4.32 to −0.64; P = .02). MVP A levels continued to de cline over the pre- diagnostic period, reaching −5.61 minutes in the matching month (95% CI, −7.35 to −3.86; P < .001) ( Supplementary T a ble 5). Sub group Differences in Pre-Diagnostic P A T rajectories Among Cases Case-only mixed- ef fects models revealed significant heterogeneity in pre- diagnostic P A trajec tories by sex, age, and BMI (Figure 3; Supplementary T a bles 6–7). Men exhibited steeper declines in both daily step counts and MVP A than w omen, supported by significa nt linear a nd quadr atic time- by-sex interaction terms (joint W ald tests, P < 0.001). P A trajec tories also varied significantly by age and BMI c ate gory (joint W ald tests, P < .001) . Participants age d ≥60 y ea rs exhibited lower over all daily step leve ls and greater reductions in daily MVP A over time. Across BMI categories, overweight and obe se participants had lower overa ll lev els of da ily steps and MVP A than those with normal BMI, and obese participants showed comparatively a ttenuated temporal de clines in both outcomes (Figures 3E a nd 3F). The underweight group was excluded fr om subgroup ana lyses because of insuffi c ient sample 13 size. Discussion Principal Findin gs In the AoU RP c ohort with linked wearable and EHR data, we found that adults who later received a n incident MDD diagnosis exhibited a mar ked, progre ssively ste epe ning decline in P A during the yea r preceding diagnosis compared with matched controls. Importantly , PA levels bega n to d evia te from indivi duals’ usual patter ns approximately 4–5 months befor e clinical diagnosis, highlighting a clinically releva nt windo w in which pe rsistent within-person downwar d traje ctorie s, rather than transient drops, may represe nt a more inform ative signal of emerging change. Thes e f indings suggest that longi tudinal, objective P A monitoring may provide c linically interpretabl e insight into functioning and psychomotor beha vior , although careful e valuation of potential confounding and subgroup heter ogeneity is warranted. Our findings extend pr io r e vidence linking lower P A to subsequent MDD diagnosis. Prior prospec tive cohort studi es [10-12, 14], including work in t he AoU RP cohort [28], have consistently associated lower P A leve ls with a higher risk of incident MDD , a pattern also observe d in our analysis, with cas es e xhibiting l ower P A than matche d controls. Beyond these established differences, our analyses revealed two key pat terns: ca ses showed significa ntly sustained dec lines in P A relative to c ont rols, and, within cases, P A deviate d from habitual levels appr oximately 4–5 months before di agnosis. Importantly , bec ause EHR-documented diagnosis likely occurs after symptom onset a nd care-seeki ng [8, 9] , the observed pre- diagnostic declines in P A should be inter preted with caution. These patterns may reflect 14 prodromal processe s [37-39], early symptomatic impairm ent, or a combination of both, rather than implying causal or temporal primacy of PA cha nges in the development of MDD. Clini ca lly , the primar y implication of longitudinal, objective PA monitoring is not to diagnose MDD, but to provide an ear ly , scalable pre- diagnosti c signal of e merging vulne ra bility i n routine care tha t may help trigger depression screening, p reve ntive strategies, or early intervention. Our f indings suggest a clinically relevant wi ndow in which sustained within- person declines in ac tivity m ay be more informative than fixed activity thresholds, which are susceptible to transient fluc tu ations arising from a range o f non- pathological factors. PA represents an actionable t arget across the course of depres sive illness, as it is both a potentially modifiable risk fac to r f or depression[6, 40, 41] and a well-established component of interve ntions that reduce depr essive symptoms among individuals with established MDD[42, 43] . Accor dingly , whether obser ved PA de clines reflect prodromal vulnerability or ear ly symptomatic impairment, timely prev ention or intervention may confer c linical benef it[10, 1 1, 42- 45], support more efficient use of healt h care resources, and reduce the broader socie tal burden of M DD [46, 47] . W e also obser ved substantial heterogen eity in pre -diagnostic P A tra jec tories by sex, age, and BMI. Declines tended to be stee per among men, reductions in hi gher -intensity activity were more pronounced a t older ag es, a nd individuals with obes ity exhibited per sistently lower activity and flatter trajectories. Sev era l facto rs may c ontribut e to these patterns, including sex differences in baseline activit y leve ls [48, 49], timing of help-seeking for mental health symptoms [50, 51], and social c ontexts of P A [52] , as wel l as age - or weight- re lated functional limitations or comorbidities that constrain higher-intensity behaviors [53]. These 15 interpre tations remain exploratory and war ra nt further inv estigation. Limitations This study has severa l limitations. F ir st, incident MDD wa s defined by the absence of EHR- documented diagnoses prior to Fi tbit monitoring, consist e nt with prior AoURP methodologies [28, 30, 31], but this definition is primarily vulnerable to left-censoring of prior disease history and may not ca pture undiagnosed cas es, warra ntin g furthe r confirmation in future studies. Se c ond, observe d pre-diagnostic declines in PA may be inf luenced by factors such as intercurrent illness, injury , c ardiometabolic disease, or medication cha nges, which are not always f ully captured o r pr ecisely timed in EHRs, limi ting the ability to fully account for these influences in the present analyses and highlighting the need for future studies with explicit control of the se covariates. Third, sel e ction bias is also possi ble, as inclusion re quired participants to have suf f iciently long Fitbi t monitoring his tories and mee t prespecified d ata completene ss criteria, pot entially limiting representa tiveness. Fourth, the study population was pre dominantly White, and the bring- your -own-device nature of Fitbit data contribution may have enriched the analyti c sa mple for more health-conscious or technologically engaged participants, pote ntially lim iting genera lizability . Conclusion s In this large cohort with linked wearable and EHR data, a dults who later rece ived an incident diagnosis of MDD exhibited sustained, within-person declines in physical activity during the year pre ce ding diagnosis, with deviations from habitua l p atter ns emer ging several months before clinica l recognition and v ar ying across demograph ic subgroups. T ogether, t hese 16 findings suggest that longitudi nal, objec tive P A monitoring using consumer w earables may offer clinically relevant early signals to support risk st ra tif ica tion, prevention, and earlier intervention for MDD , whil e unde rscoring the need for ca ref ul consid er a tion of confounding and subgroup he terogeneity . 17 Acknowledgments W e gra t ef ully acknowledge All of Us participants for their contributions, without whom this researc h would not have been possible. W e also thank the National Institut es of Health’ s A ll of Us Research Program for making available the participant data e xamined in this study . Fundin g Richard JB Dobson is supported by the following: (1) Nati onal Institute for H ealth and Care Research (NIHR) Biomedical Research Centre (BRC) at South London and Maudsley National Health Service (NHS) Foundation T r ust and King’ s College London; (2) Health D a ta Research UK, w hi ch is funde d by the UK Medical Rese arch Council (MRC), Engineer ing and Physical Sciences Research Council, Economic a nd Soci al Research Council, Department of Hea lth and Social Care (England), Chief Sci entist Office of the Scottish Gover nment Health and Social Care Dire ctora tes, Health and Social Car e Research and Development Division (W elsh Government), Public Health Age n cy ( Northern Irel and) , British Heart Foundation, and W ellcome T rust; (3) the BigData@Heart Consortium, funded by the I nnovative Medicines Initiative 2 Joint Undertaking (whic h re ce ives support fro m the EU’ s Horiz on 2020 research and innovation progra mme and European Fed eration of Pharmaceutica l Indust ries a nd Associations [EFPIA], par tn ering with 20 acade mic and i ndustry pa rtner s and Eur opean Society of Cardiology); (4) the NIHR Unive rsity College London Hospitals BRC ; (5) the NIHR BRC at S outh London and Ma udsley (re lated to attendance at the American Medical Informa tics Assoc iation) NHS F oundation T r ust and King’ s College London; ( 6) the UK Research a nd Innovation (UKRI ) London Me dical Imagi ng & Ar tificial Intelli genc e Centre 18 for V alue Based Healthcare (AI 4VBH); (7) the NIHR Appl ied Resea rch Collaboration (ARC) South London at King’ s College Hospital NHS Foundation T rust; a nd (8) W ellcome T rust. The funders had no r ol e in the de sign and conduct of the s tudy; collec tion, manageme nt, analysis, and interpretation of the d ata ; preparation, revi ew , or a pproval of the manuscript; and dec ision to submi t the manuscr ipt for publication. Conflicts of Interest Abhishek Pratap is an employee of Boehringer Inge lh eim Pharmaceutica ls, Inc., Ridgefield, CT , USA. Amos Folarin and Richa rd JB Dobson ar e cofounders of Onsentia. Amos Folarin holds shares of G oogl e. Data A vailability T o e nsure participant privacy , the data used in this study a r e a vailable to app rove d researchers through the All of U s Research W orkbench (https://workb ench.researc hallofus.or g/login) following registration, completion of required ethics training, and atte station of a data use agreement. Public release of individual-leve l participant d ata is not per mitted under the All of Us Research Program privac y polici es. Authors’ C ontribution s YZ had f ull acc ess to all study data a nd takes responsibility for the integrity of the data and the accuracy of th e da ta analysis. YZ, AF , and RJBD contributed to the study conc ept and design. Data acquisition, analysis, or interpretation were performed by YZ, AF , AP , HLE, RZ, CS, HS , HK, S S, and RJBD. Y Z dra fted the manuscript and conducted the statistical analysis. 19 Funding was obtained by RJBD and A F . All authors c ritically reviewed the manuscript for important intellectual content. Abbr eviations AoURP: A ll of Us Research Program BMI: body mass index CI: confidence interval EHR: electronic health r ec ord ICD: Interna tional Classific ation of Disea ses IQR: interquartile range MET : metabolic e quivalent of task MDD: major depressive disorder MVP A: modera te- to -vigorous physical activity OMOP: Observational Medical Outcome s Pa rtner ship P A: physical a ctivity SMD: standardized mean difference 20 References: 1. V os T , Lim SS, Abbaf ati C, Abbas KM, Abbasi M, A bbasifard M, et al. Global burd en of 369 diseases a nd injuries in 204 countrie s and territories, 1990–2019: a systematic ana lysis for the G lobal Burd en of Disease Study 2019. The lancet. 2020;396(10258):1204-22. 2. W alker ER, McGee RE, Druss B G. Mortality in mental disorders a nd global disease burden implications: a systematic review and meta -analysi s. JAMA psyc hiatry . 2015;72(4):334-41. 3. Cambridge OR, Knight MJ, Mill s N, Baune BT . The clinical relationship between cognitive impairment and psyc hoso cia l functioning in ma jor depr essive disorder: a systematic review . Psychiatry research. 2018;269:157-71. 4. V ancampfort D, Correll CU, Galling B, P robst M, De H ert M, W a rd PB, et al. Diabe tes mellitus i n people with schizophre nia, bipolar disorder an d major depressive disorde r: a systematic review and la rg e scale meta‐analysis. W or ld psychiatry . 2016;15(2):166 -74. 5. Patel V , Chisholm D, Parikh R, Charlson FJ, Degenha rdt L, Dua T , e t al. A ddressing the burden of mental, neurological, and substance use disord ers: key message s from Disease Control Priorit ies. The Lanc et. 2016;387(10028):1672-85. 6. Firth J, S olmi M, W oot ton RE, V anc ampfort D, Schuc h F B, Hoare E, et al. A meta‐ review of “lifestyle psy chia try”: the role of exercise, smo king, diet and sleep in the preve ntion and treatment of mental disorders. W orld psyc hiatry . 2020;19(3):360- 80. 7. Kraus C, Ka driu B , Lanzenbe rg e r R, Zarate Jr CA, Kasper S. Prognosis and im prove d outcomes in major depression: a re vi ew . T ranslational psychiatry . 2019;9(1) :127. 8. Koze y SL, L yden K, H owe CA, St aude nmayer JW , Freedson PS . Ac ce lerometer output and MET values of common physical activi ties. Medicine and scie n ce in sports and exercise. 2010;42(9):1776. 9. Gurrieri R, Russom anno G , Gambini M, Pescini E, Sit à G, Ma razziti D. The Duration of Untrea t ed I llness in Major Depressive Disorder: Clinical Relevance, Pre dictors, and Strategies for Early Intervention. Psychiatry Research Co mmunications. 2025:100231. 10. Schuch FB, V a nca mpfort D, Firth J, Rosenbaum S, W ard PB , Silva ES, et a l. Physical activity and incident de pression: a meta-analysis of prosp ective c ohort st udies. A merican journal of psychia try . 2018;175(7):631-48. 1 1. Pearce M, Garcia L, Abbas A, Strain T , Schuch FB , Golubic R, et al. Association betwee n physi ca l activit y and r isk of depression: a systematic re vi ew a nd meta-ana lysis. JAMA psyc hiatry . 2022;79( 6):550-9. 12. Bizzozero- Peroni B, Díaz-Goñi V , Ji ménez-López E, Rodríguez-Gutiérrez E, Se quí- Domínguez I, de Arena s-Arroyo SN, et al. Daily st ep count and depression in adults: a systematic review and me t a -analysis. JAMA Networ k Open. 2024;7(12):e2451208- e. 13. Aze vedo Da Silva M, Si ngh-Ma noux A, Brunner EJ, Kaffashian S, S hipley MJ, Kivimäki M, et al. Bidirectional associa tion between phys ical a ctivity and symptoms of anxiety and de pression: the Whitehall II study . European journal of epidemiology . 2012;27(7):537-46. 14. Qu S, Xing Z. Dose-response relationship between acce l erometer-measured physical activity and depression: evidence fr om the UK Bi obank. T r anslational Psychiatry . 2025;15(1):297. 15. Wüthrich F , Nabb CB, Mittal V A, Shankma n SA, W alther S. A ctigraphically measured 21 psychomotor slowing in depression: systematic re vi ew a nd meta-a nalysis. P syc hological medicine. 2022;52(7) :1208-21. 16. Mohr DC, Zhang M, Schueller SM. Person al sensing: understanding menta l health using ubiquitous sensors and machine learning. Annual review of clinical psychology . 2017;13(1):23-47. 17. Zapata-La mana R, Lalanza JF , Losilla J-M, Parrado E, Ca pdevila L. mHealth technology for ecological momentary assessment in physica l ac tivity research: a systematic review . PeerJ. 2020;8:e8848. 18. De Angel V , Le wis S, White K, Oe tzmann C, Leightley D, Opre a E, e t al. Digital health tools for the passive monitoring of depression: a systematic review of methods. NPJ digit al medicine. 2022;5(1) :3. 19. V allance JK, W inkler EA , Ga rdiner P A, Healy GN, L ynch BM, Owen N. Associations of objectively-a ssessed physical ac tivity and sedentary time with depre ssion: NHANES (2005 – 2006). Preve ntive medi cine . 201 1;53(4 -5):284-8. 20. Zhang Y , Stewart C, Ranjan Y , Conde P , Sankesara H, Ra shid Z, et al. Large- scale digital phenotyping: identifying depression and a nxiety indi ca tors i n a ge neral UK population with over 10,000 participants. Journa l of Affective Disorders. 2025; 375:412 -22. 21. Investigators AoUR P . The “All of Us” research program. Ne w England Journal of Medicine. 2019;381(7) :668-76. 22. Mayo KR, Basford MA, Carroll RJ, Dillon M, F ullen H , Leung J, et a l. The All of Us Data a nd R ese arch Center: creating a secure, scalable, an d sustaina ble ec osystem for biomedical re search. Annual review of biomedical da t a science . 2023;6(1):443-64. 23. Master H, K ouame A, Marginean K, Basford M, Harris P , Holko M, editors. How Fitbi t data are be ing made available to r egistere d researchers in A ll of Us Research Program. P ACIFIC SYMPOSIUM ON BIOCOMPUTING 2023: Kohala Coast, Hawaii, USA, 3 –7 Januar y 2023; 2022: W orld Scientific. 24. T udor-Locke C, Craig CL, Brown WJ, Clemes SA, De Cocker K, Giles -Corti B, et al. How many steps/day are enough? For adults. International Journal of Behavioral Nutrition and Physical Ac tivity . 201 1;8(1):79. 25. Bull FC, A l-Ansar i SS , Biddle S, Borodulin K, B u man MP , Car don G, et al. W orld Hea lth Org a nization 2020 guidelines on physical activity and sedentary behaviour . British journal of sports medicine . 2020;54(24):1451-62. 26. Semanik P , Lee J, Pellegrini CA, Song J, Dunlop DD, Chang R W . Comparison of physical ac tivity measures de rived f rom the Fitbit F lex and the Ac tiGraph GT3 X+ in an employee popula tion with chroni c knee symptoms. ACR open rheumatology . 2020;2(1):48 - 52. 27. Brewer W , Swanson BT , O rtiz A . V alidity of Fitbit’ s a ctive minutes as compared w ith a researc h-grade acce lerometer and self-reported measures. BMJ open sport & exercise medicine. 2017;3(1) . 28. Master H, Annis J, Huang S, Beckman JA, Ratsimbazaf y F , Marginean K, et al. Association of step c ounts over ti me with the risk of c hro nic disease in the All of Us Research Program. Nature medicine . 2022;28 (1 1):2301- 8. 29. Brittain EL, Han L, A nnis J, Master H, Hugh es A , Roden DM, et al. Physi ca l activity and incident obesity acr oss the spectrum o f ge netic risk for obesit y . JAMA Ne twork Ope n. 22 2024;7(3):e243821- e. 30. Y akdan S, Benedic t B, Si ngh P , Frumkin MR, Goodin BR, Ne uman B, et al. Association of ac tivity with t he risk of de veloping musculoskeletal pai n in the A ll of Us research program. The Journa l of Pain. 2025:105516. 31. Zheng NS, Annis J, Master H, Han L, Gl eic hauf K, Ching JH, e t al. Sleep patterns and risk of chr onic dis ea se as measured by long-term monitoring with commercial wearable device s in the A ll of Us Research Program. Nature m edicine. 2024;30(9):2648 -56. 32. Klann JG, Joss MA, Embree K, Murphy SN. Dat a model harmonization for the All Of Us Research Program: T r ansfor ming i2b2 data into the OMOP common data mode l. PloS one. 2019;14(2):e 0212463. 33. W agner M, Helmer C, Tzourio C, Berr C, Proust-Lima C, Samieri C. Evaluation of the concurrent tra jectori es of car diometabolic risk fa ctors in the 14 ye ars before dementia. JAMA psychiatry . 2018;75(10):1033-42. 34. W u Z, Cr ibb L, W olfe R, Shah RC, Orcha rd SG, Owen A , et al. Cardiometabolic trajec tories preceding d ementia in Community-Dwe lling older individuals. JAMA network open. 2025;8(2):e 2458591- e. 35. Jia J, Ning Y , Chen M, W a ng S, Y ang H, Li F , e t al. Biomar ker changes during 20 years preceding A lzheimer ’ s disea se. New England Journal of Medicine. 2024;390(8):712 - 22. 36. Benjamini Y , Hochbe rg Y . Controlling t he f alse discove ry rate: a practical and powerful approach to multiple testing. Journal of the Royal statistical society: series B (Methodological). 1995;57( 1 ):289- 300. 37. Pede VB, Jaiswal SV , S awa nt V A. Study of prodromal a nd residual symptom s of depre ssion. Industrial psy chiatr y journal. 2017;26(2):121-7. 38. Iac ovi ello BM, Alloy LB, Abra mson L Y , Choi JY . The early course of depression: a longitudinal investi gation of pr odromal symptoms and the ir relation to the symptom atic course of depressive episodes. Journal of abnorma l psychol ogy . 2010;1 19(3):459. 39. Benasi G, Fava GA , Guidi J. Prodromal symptoms in depression: a systematic review . Psychotherapy a nd psychosomatics. 2021;90(6):365-72. 40. de Pablo GS, Solm i M, V aquer izo- Serrano J, Radua J, Passina A, Mosillo P , e t al. Primary prevention of depression: an umbrella review of controlled interventions. Journal of affective disorders. 2021;294:957-70. 41. Hallgren M, Stubbs B, V anca mpfort D, Lundin A, Jääkalli o P , Forsell Y . T rea tment guidelines for de pression: gre ate r emphasis on physical activit y is neede d. European Psychiatry . 2017;40:1-3. 42. Schuch FB, V a nca mpfort D, Richards J, Rosenbaum S, W ard PB, Stubbs B . Exer cise a s a treatment f or depression: a meta -analysis adjusting for publi ca tion bias. Journal of psychiatric researc h. 2016;77:42-51. 43. Kandola A, A shdown-Franks G, Hendrikse J, Sabiston CM, S tubbs B. Physical ac tivity and depression: T owards understanding the a ntidepressan t mecha nisms of physical activity . Neurosc i ence & Biobehaviora l Reviews. 2019;107:525-39. 44. Mammen G, Faulkner G . Physic al ac tivity and the preventi on of depr ession: a systematic review of prospective studi es. American journal of prev entive medicine. 2013;45(5):649 - 57. 45. T e ychenne M, Ball K, Salmon J. Physi cal a ctivity and likelihood of depression in adults: a re vi ew . Preve ntive m edic ine. 2008;46(5):397-41 1. 23 46. W ang PS, Si mon G, Kessler RC. The ec onomic burden of depression and the cost‐ effectiveness of treatment. International journal of m ethods in psychiatric r esearch. 2003;12(1):22-33. 47. Le LK-D, Esturas AC, Mihalopoulos C, C hiotelis O, Buc holc J, Chatterton ML, et al. Cost-effectiveness evidence of mental h ea lth prevention a nd promotion interventions: A systematic review of economic e valuations. P LoS medicine. 2021;18(5):e 1003606. 48. Casperse n CJ, Per eira MA, Curran KM. Changes in physi ca l activity patterns in the United States, by sex and cross- sectional age. Medicine & science in sports & exercise. 2000;32(9):1601-9. 49. Guthold R, S tevens GA , Riley LM, Bull FC. W or ldwide tr ends in insufficient physical activity from 2001 to 2016: a pooled a nalysi s of 358 population- based sur veys with 1· 9 milli on par ticipants. The la ncet global health. 2018;6(10):e1077-e 86. 50. Seidler ZE, Dawes AJ, Rice SM, Olif fe JL, Dhillon HM. The role of masculinity i n men's help-see king for depression: a systematic re view . Clini ca l psychology re view . 2016;49:106- 18. 51. Y ousaf O, Gr unfeld EA, Hunter MS. A systematic r eview of the f actors associated with delays in medica l and psyc hological help-seeking among m en. He alth psychology review . 2015;9(2):264-76. 52. Aze vedo MR , A raújo CLP , Reichert FF , Siqueira FV , da Silva MC, Hallal PC . Gende r differences in leisure-time physical activity . Inter n ational journa l of public health. 2007;52(1):8. 53. Baillot A, Che nail S, Barros Polita N, Si monea u M, Libourel M, Nazon E, et a l. Physi ca l activity motives, barrier s, and pr ef erences in peopl e w ith obesity: A systematic r eview . PloS one. 2021;16(6):e 02531 14. 24 T able 1. Characteristics of Incident Major Depressive Disorder C ases and Matched Cont rols. Characteristics Overall (N = 4104) Case (n = 829) Contr ol (n = 3275) SMD a Age b , median [IQR], y 48.4 [36.3, 61.3] 48.4 [36.2, 61.2] 48.4 [36.3, 61.4] 0.004 BMI c , median [IQR] 29.9 [25.6, 34.9] 29.8 [25.6, 35.4] 29.9 [25.7, 34.7] 0.046 W omen, n (%) 3355 (81.7) 676 (81.5) 2679 (81.8) 0.033 Race, n (%) 0.098 White 3384 (82.5) 691 (83.4) 2693 (82.2) Black or African Ame rican 271 (6.6) 40 (4.8) 231 (7.1) Other d 449 (10.9) 98 (1 1.8) 351 (10.7) Ethnicity , n (%) 0.025 Hispanic or Latino 267 (6.5) 56 (6.8) 21 1 (6.4) Not Hispanic or Latino e 3837 (93.5) 773 (93.2) 3064 (93.6) Abbreviations: BMI, body mass index; IQR, interquartile range ; SMD, standa rdized mean dif ference. a SMDs are presented as absolute values; values le ss than 0.1 indicate negligible imbalance between groups. b Age was de fined at the di agnosis month for cases and the m atched index month for contr ols. c BMI was derived from measurements closest to one year befor e the diagnos is or matching month to minimize potential influence of emerging major depress ive diso rder on body weight. d Participants with missing, unknown, or less frequently reported r ace c ategories were grouped into the “Other” category in accordance with All of Us data reporting pol icies. e Participants with missing or unknown ethnicity were grouped wit h the “Not Hispa nic or Latino” category in accordance w ith All of Us data reporting policies. 25 T able 2. Linear Mixed-Eff ects Model Comparing Pr e -diagnostic Tr ajectories of Daily Step Counts and Moderate- to -V igorou s Physical Ac tivity (MVP A ) Between Incident MDD Cases and Contr ols. T erm Estimate (95% CI) T erm P value Global T rajectory T est ( P V alue) a Daily step count mode l (unit: steps) b,c,d,e <.001 Intercept 8249.57 (8130.24 to 8368.90) <.001 group × case − 1109.57 ( − 1373.76 to − 845.39) <.001 time 3.66 ( − 1 1.58 to 18.90) .64 time × case − 92.08 ( − 126.14 to − 58.02) <.001 time ² 1.07 ( − 0.16 to 2.30) .09 time ² × ca se − 5.47 ( − 8.23 to − 2.70) <.001 MVP A model (unit: minutes) <.001 Intercept 58.69 (56.82 to 60.55) <.001 group × case − 11.35 ( − 15.48 to − 7.22) <.001 time 0.05 ( − 0.23 to 0.32) .75 time × case − 0.78 ( − 1.39 to − 0.18) .01 time ² 0.02 ( − 0.00 to 0.04) .08 time ² × ca se − 0.04 ( − 0.09 to 0.01) .10 a The global trajectory test (joint W ald test) evaluates whether o verall phys ical activity trajectories differ between cases and contr ols by jointly testing the interaction term s (time × ca se and time² × case). b T ime was modeled on a retrospective monthly scale from −12 to 0 months relative to the diagnosis (or matching) month. c The intercept represents the estimated mean physical acti vity level for the reference group (contr ols) at the reference time point (month 0) . d Group × case repre sents the baseline di fference between incident major depressive dis order cases and matched controls (case –control status). e T ime × case and time² × case represent dif ferential linear and quadratic changes trajectories between cases and controls over time. 26 Figur e 1. Study Flowchart f or the Identification of Inci dent MDD Cases and Matc hed Controls 27 Figur e 2. T r ajectories of Daily Step Counts (A) and Mod erat e- to -V igorous Physi cal Activity (MVP A) (B) Pre ce din g Incident MDD D iagnosis. 28 Figur e 3. Subgr oup-S pecific T r ajectories of Physi cal Activity Pr eceding In cident MDD Diagnosis. (A) Daily Step Count T ra jec tories by Sex. (B) Moderate- to - V igorous Physical Activity (MVP A) T r ajec tories by Sex. (C) Daily S tep Count T r ajec tories by Age. (D) MVP A T ra jector i es by Age. (E) Daily Step Count T ra jectorie s by Body Mass Inde x (BMI). ( F) MVP A T r ajec tories by BMI.
Original Paper
Loading high-quality paper...
Comments & Academic Discussion
Loading comments...
Leave a Comment