Artificial intelligence-enabled single-lead ECG for non-invasive hyperkalemia detection: development, multicenter validation, and proof-of-concept deployment
Hyperkalemia is a life-threatening electrolyte disorder that is common in patients with chronic kidney disease and heart failure, yet frequent monitoring remains difficult outside hospital settings. We developed and validated Pocket-K, a single-lead …
Authors: Gongzheng Tang, Qinghao Zhao, Guangkun Nie
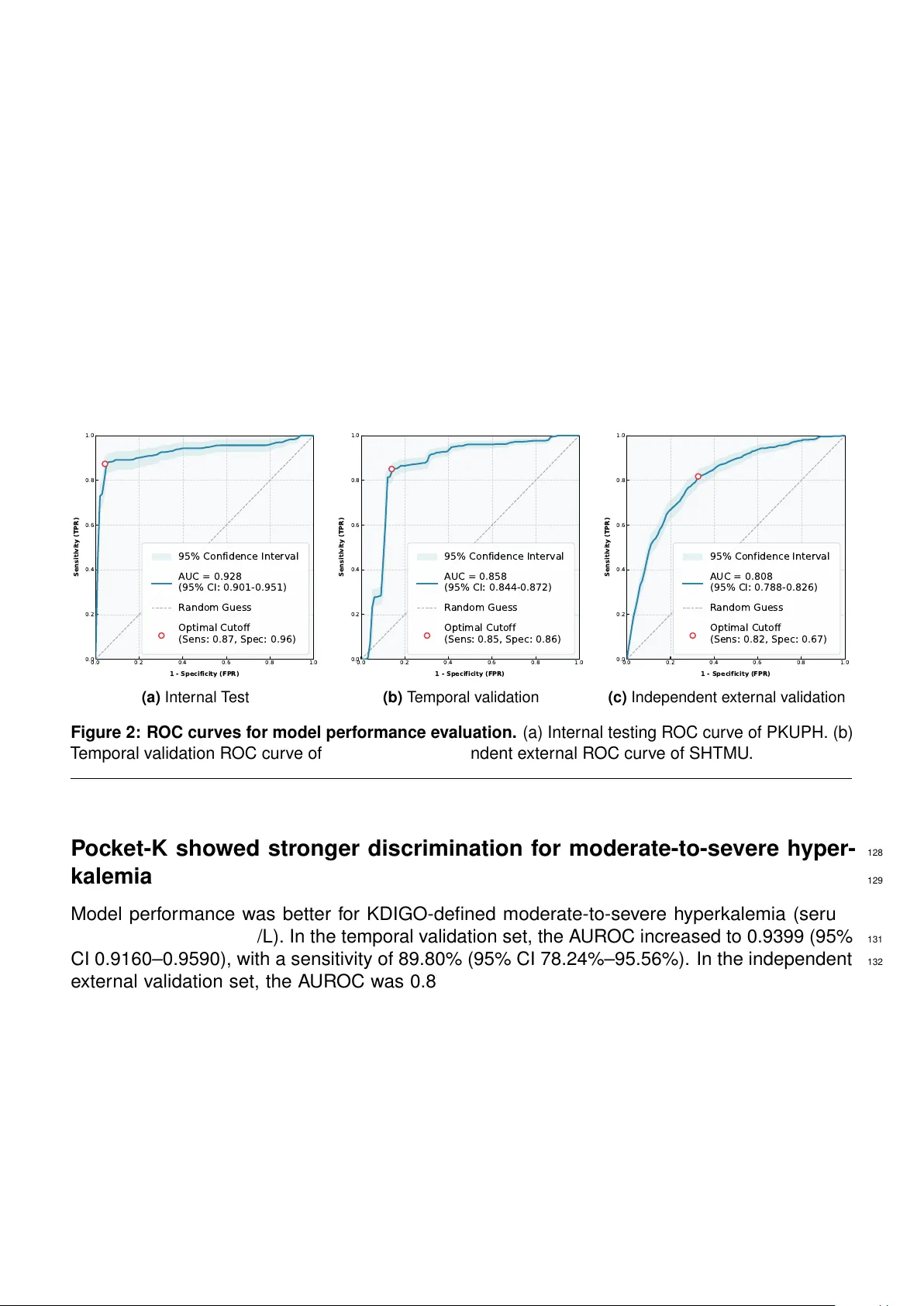
Artificial intellig ence-enabled single-lead ECG f or non-in v asive hyperkale mia detection: 1 development, m ulticenter v alidation, and proof-of-concept deplo yment 2 Gongzheng T ang 1,2,#, , Qinghao Zhao 3,# , Guangkun Nie 4,# , Y ujie Xiao 1,2 , Shijia Geng 5 , Donglin 3 Xie 1,2 , Shun Huang 2 , Deyun Zhang 5 , Xingchen Y ao 6,7,8 , Jinwei W ang 6,7,8 , Kangyin Chen 9,* , Luxia 4 Zhang 2,6,7,8,* , and Shenda Hong 1,2,10,11,*, 5 1 Institute of Medical T echnology , P eking Univ ersity Health Science Center , Beijing, China 6 2 National Institute of Health Data Science, P eking Univ ersity , Beijing, China 7 3 Depar tment of Cardiology , P eking University P eople’ s Hospital, Beijing, China 8 4 School of Intelligence Science and T echnology , P eking Univ ersity , Beijing, China 9 5 Hear t V oice Medical T echnology , Hefei, China 10 6 Renal Division, Depar tment of Medicine, P eking University First Hospital, Beijing, China 11 7 Institute of Nephrology , Ke y Laboratory of Renal Disease, Ministr y of Health of China, and K ey 12 Laboratory of Chronic Kidney Disease Pre vention and T reatment (P eking University), Ministry of 13 Education, Beijing, China 14 8 Research Units of Diagnosis and T reatment of Immune-mediated Kidne y Diseases, Chinese 15 Academy of Medical Sciences , Beijing, China 16 9 Tianjin K e y Laboratory of Ionic-Molecular Function of Cardiovascular Disease , Depar tment of 17 Cardiology , Tianjin Institute of Cardiology , The Second Hospital of Tianjin Medical University , 18 Tianjin, China 19 10 State K e y Laboratory of V ascular Homeostasis and Remodeling, NHC K ey Labor ator y of 20 Cardiov ascular Molecular Biology and Regulatory P eptides, P eking Univ ersity , Beijing, China 21 11 Institute f or Ar tificial Intelligence, P eking University , Beijing, China 22 # These authors contributed equally 23 * Correspondence: hongshenda@pku.edu.cn, zhanglx@bjmu.edu.cn, chenkangyin@vip .126.com 24 ABSTRA CT 25 Hyperkalemia is a life-threatening electrolyte disorder that is common in patients with chronic 26 kidney disease and hear t f ailure , y et frequent monitoring remains difficult outside hospital settings. 27 W e de veloped and validated P oc k et-K, a single-lead AI-ECG system initialized from the ECG- 28 F ounder f oundation model for non-in v asiv e hyperkalemia screening and handheld deployment. In 29 this multicentre observational study using routinely collected clinical ECG and labor ator y data, 30 34,439 patients contr ib uted 62,290 ECG–potassium pairs. Lead I data were used to fine-tune the 31 model. Data from P eking Univ ersity P eople’ s Hospital w ere divided into de v elopment and tempor al 32 v alidation sets, and data from The Second Hospital of Tianjin Medical Univ ersity ser ved as an 33 independent e xternal validation set. Hyper kalemia was defined as v enous serum potassium > 5 . 5 34 mmol/L. P oc k et-K achiev ed A UR OCs of 0.936 in inter nal testing, 0.858 in temporal validation, 35 and 0.808 in e xternal validation. F or KDIGO-defined moderate-to-se v ere h yperkalemia (serum 36 potassium ≥ 6.0 mmol/L), A UROCs increased to 0.940 and 0.861 in the temporal and e xter nal 37 sets, respectiv ely . Exter nal negative predictiv e v alue e xceeded 99.3%. Model-predicted high risk 38 below the h yperkalemia threshold was more common in patients with chronic kidney disease 39 and hear t f ailure. A handheld prototype enab led near-real-time inf erence, suppor ting future 40 prospectiv e e valuation in nativ e handheld and wearable settings . 41 1 INTR ODUCTION 42 Hyperkalemia, defined as a venous ser um potassium concentration abov e 5.5 mmol/L, is a 43 common and potentially fatal electrolyte abnor mality and a major r isk f actor for malignant ar- 44 rh ythmia and sudden cardiac death 1 . It is par ticular ly common in patients with chronic kidney 45 disease and hear t f ailure, and its incidence increases substantially as renal function declines 2,3 . 46 Pre vious studies ha v e repor ted a U-shaped association between potassium concentration and 47 mor tality , with h yperkalemia linked to a higher risk of death in chronic kidne y disease , hear t f ailure, 48 and acute my ocardial inf arction 4–6 . Timely inter v ention theref ore depends on r apid and reliable 49 recognition. 50 Confir mation of h yperkalemia currently relies on venous b lood sampling and laborator y mea- 51 surement of potassium. Although this standard is accurate , it is inv asive , inter mittent, and 52 dependent on access to clinical f acilities, limiting frequent monitoring between routine visits f or 53 high-risk patients 7 . Hyperkalemia also produces character istic electrocardiographic changes, 54 including peaked T w a ves and QRS widening, which mak es the electrocardiogr am a plausible 55 non-inv asiv e screening tool 8 . Howe ver , visual inter pretation alone has limited sensitivity , ev en 56 among e xperienced clinicians , which reduces the reliability of the electrocardiogr am f or screening 9 57 and leav es hyperkalemia management an ongoing clinical challenge. 58 Ar tificial intelligence (AI), par ticular ly deep lear ning, has been increasingly applied in clinical 59 research and cardiov ascular medicine 10–16 . In electrocardiograph y , AI-based methods can detect 60 subtle wa v ef or m features that are difficult to recognise by routine visual inspection and hav e 61 shown promise in identifying cardio vascular and metabolic abnor malities 17–21 . In hyperkalemia, 62 models trained on standard 12-lead ECGs ha ve sho wn strong diagnostic perf ormance and can 63 capture risk signals that are subclinical or missed b y con v entional inter pretation 22–24 . Howe v er , 64 the workflow required to acquire a 12-lead ECG limits its use f or repeated sur veillance and 65 self-screening outside the hospital, where scalable monitoring may be most v aluable f or high-risk 66 patients. By contrast, single-lead ECG, par ticularly Lead I, is the dominant f ormat used b y 67 handheld recorders and smar twatches , making it well suited to home monitoring and out-of- 68 hospital screening. Small single-centre studies from the USA, T aiw an, and other settings ha v e 69 provided early evidence that single-lead h yperkalemia detection is f easible 25–27 . How e ver , the 70 current e vidence base remains limited by modest sample size , restr icted population div ersity , and 71 the absence of r igorous large-scale multicentre v alidation. Consequently , performance across 72 heterogeneous populations, diff erent health systems and acquisition platf or ms, and real-w orld 73 pre v alence settings remains uncer tain. 74 W e theref ore de v eloped P ock et-K, a single-lead AI-ECG model f or h yperkalemia screening, 75 initialised from a pretr ained ECG f oundation model. We e valuated model perf or mance in three 76 settings: inter nal testing within the de v elopment set, tempor ally separated v alidation within the 77 same health system, and independent e xter nal validation in a second health system using a 78 diff erent ECG platf or m. We also e xamined wav eform-lev el inter pretability , patient-le v el longitudinal 79 trajectories, clinical phenotypes associated with false-positiv e predictions, and the technical 80 f easibility of handheld deplo yment. 81 RESUL TS 82 Study Overvie w 83 W e de v eloped P oc k et-K, a single-lead ECG model for non-in v asiv e hyperkalemia screening that 84 was initialized from a pretrained ECG f oundation model. The ov erall study design is shown in 85 Figure 1. The study used a multistage design. W e first constructed ECG– K + pairs by linking 86 2 each ECG to a v enous ser um potassium measurement obtained within a ± 1-hour window . We 87 then fine-tuned the pretrained foundation model, ECGF ounder , to estimate the probability of 88 h yperkalemia, defined as ser um K + > 5 . 5 mmol/L. 89 W e e v aluated the model in 34,439 unique patients from two independent health systems. At the 90 primar y site , P eking University P eople’ s Hospital(PKUPH), patients were divided chronologically at 91 July 2021 to e xamine perf ormance ov er time, yielding a de v elopment set ( N = 10 , 409 ; n = 26 , 145 92 pairs) and a tempor al v alidation set ( N = 5 , 054 ; n = 10 , 922 pairs). We then tested the model in 93 an independent e xter nal v alidation set from The Second Hospital of Tianjin Medical Univ ersity 94 (SHTMU) ( N = 18 , 976 ; n = 25 , 223 pairs), which included different ECG management systems, 95 hardware en vironments, and care settings . 96 W e also conducted a proof-of-concept ev aluation to assess whether the model could suppor t 97 near-real-time, out-of-hospital screening in high-risk populations using handheld single-lead 98 de vices. This study design allowed us to e valuate P ock et-K both in histor ical clinical datasets and 99 in a practical prototype deplo yment setting. 100 ECGFo u n d er Pretrained Foundation Model 30-s ec L ead I ECG Real -t i m e In f er en c e In s t an t Ri s k A l er t I. Dev el o p m en t 26,145 ECG-K+ pairs Development cohort (PKUPH) Fine-tune dataset Physiologically anchored ECG-K+ pairing ± 1h Lead I ECG Venous serum K + Po c k et -K Fine-tuned Model II. Val i d at i o n Temporal Validation (PKUPH) Independent External Validation (SHTMU) TMUSH N = 18,976 J an 2024-Dec 2024 PK UPH N = 5,054 A u g 2021-No v 2024 Internal Test (PKUPH) PK UPH N = 1,041 J an 2016-Ju l 2021 from Development Set III. Pr o o f -o f -c o n c ep t d ep l o y m en t Figure 1: Overview of P oc ket-K de v elopment, validation, and proof-of-concept deployment. In the dev elopment stage, ECG– K + pairs were constructed by linking each ECG to the nearest eligible v enous serum potassium measurement within a ± 1-hour windo w . These paired data were used to fine-tune ECGF ounder , a pretrained ECG f oundation model, to de v elop P oc k et-K. In the v alidation stage, model performance was assessed in three settings: an inter nal test set from the PKUPH de v elopment set, a temporal v alidation set at PKUPH, and an independent e xter nal v alidation set from SHTMU . In the proof-of-concept stage, a handheld de vice recorded a 30-s lead I ECG, which was processed through a smar tphone-based workflow f or near-real-time inf erence and generation of a h yperkalemia risk aler t. Study population and baseline c haracteristics 101 The final study population included 34,439 unique patients and 62,290 ECG– K + pairs from two 102 health systems. After quality control at PKUPH, 15,463 patients contr ibuted 37,067 eligib le pairs. 103 Of these, 10,409 patients with 26,145 pairs f or med the dev elopment set, and 5,054 patients with 104 3 10,922 pairs f ormed the temporal v alidation set after e xclusion of patients who o verlapped with 105 the de v elopment set. SHTMU contributed 18,976 patients with 25,223 pairs for independent 106 e xter nal v alidation. 107 Baseline clinical char acteristics and technical specifications are summarised in T ab le 1. Across 108 sets, mean age ranged from 54.08 to 58.25 years , and men accounted f or 53.3%–56.0% of 109 patients. Compared with the dev elopment set, the e xter nal validation set had a higher burden 110 of renal dysfunction and cardiorenal comorbidity . In all sets, the mean inter v al between ECG 111 acquisition and potassium measurement was less than 30 min, suppor ting close ph ysiological 112 alignment between w av ef orm acquisition and the laborator y ref erence. 113 T able 1: Baseline clinical characteristics, ECG–potassium pairing quality , and technical specifi- cations across study sets. Continuous variab les are presented as mean (SD), and categor ical v ariables as n (%). PKUPH: P eking University P eople’ s Hospital; SHTMU: The Second Hospital of Tianjin Medical Univ ersity; K + : serum potassium; eGFR: estimated glomer ular filtration rate; ECG: electrocardiogram. Characteristic Development Set (PKUPH) T emporal V alidation Set (PKUPH) Independent External V alidation Set (SHTMU) ( N = 10 , 409 ; n = 26 , 145 ) ( N = 5 , 054 ; n = 10 , 922 ) ( N = 18 , 976 ; n = 25 , 223 ) Demographics Age, y ears 54.08 (15.55) 54.60 (14.70) 58.25 (17.90) Male se x, n (%) 5,642 (54.2%) 2,830 (56.0%) 9,994 (53.3%) Laboratory measurements Serum K + , mmol/L 4.14 (0.36) 4.19 (0.40) 4.11 (0.42) Serum creatinine, µ mol/L 74.66 (95.29) 78.68 (173.15) 106.08 (380.26) eGFR, mL/min/1.73 m 2 95.80 (23.14) 93.84 (21.91) 93.92 (28.84) eGFR-based categories, n (%) ≥ 90 8,757 (84.1%) 3,915 (77.5%) 12,523 (66.0%) 60–89 1,291 (12.4%) 932 (18.4%) 4,418 (23.3%) 30–59 242 (2.3%) 143 (2.8%) 1,241 (6.5%) < 30 119 (1.1%) 64 (1.3%) 794 (4.2%) ECG–potassium pairing quality ECG-to- K + inter v al, min 28.46 (14.88) 24.44 (14.41) 22.39 (16.26) Comorbidities, n (%) Hyper tension 2,263 (21.7%) 1,453 (28.7%) 6,778 (35.7%) Diabetes mellitus 1,041 (10.0%) 690 (13.7%) 3,137 (16.5%) Chronic kidney disease 430 (4.1%) 238 (4.7%) 2,127 (11.2%) Hear t f ailure 68 (0.7%) 57 (1.1%) 437 (2.3%) Coronar y ar ter y disease 765 (7.3%) 556 (11.0%) 2,463 (13.1%) Stroke 444 (4.3%) 262 (5.2%) 1,357 (7.2%) T echnical specifications ECG management system MedEx MedEx Nalong Dominant hardware GE / Philips GE / Philips Nalong / Nihon K ohden Sampling frequency , Hz 500 500 500 / 1000 N denotes the number of unique patients, and n denotes the number of ECG–potassium pairs . T echnical specifications are repor ted at the set le vel r ather than the patient le vel. 4 P ocket-K generalized across internal, temporal, and independent e xternal 114 v alidation sets 115 P ock et-K showed stable discr imination across the validation sets. In the inter nal test set, the 116 A UROC was 0.9364 (95% CI 0.9135–0.9575), with a sensitivity of 83.33% (95% CI 78.24%– 117 87.43%) and a specificity of 96.60% (95% CI 96.06%–97.07%) at the prespecified frozen threshold. 118 In the temporal v alidation set, despite changes in case mix o v er time, the A UROC w as 0.8582 119 (95% CI 0.8441–0.8723), with a sensitivity of 85.05% (95% CI 81.84%–87.77%), suggesting 120 robustness to temporal drift. In the independent e xter nal set, the A UR OC was 0.8076 (95% CI 121 0.7883–0.8258) despite concurrent diff erences in ECG platf or m and lo wer disease pre v alence, as 122 shown in Figure 2. 123 Although discr imination decreased across increasingly heterogeneous e valuation settings , the 124 negativ e predictive v alue remained high and e xceeded 99.3% in the e xter nal set. These findings 125 suppor t the role of P ock et-K as a rule-out screening tool f or identifying low-risk states rather than 126 a replacement f or laboratory confir mation. 127 0.0 0.2 0.4 0.6 0.8 1.0 1 - Specificity (FPR) 0.0 0.2 0.4 0.6 0.8 1.0 Sensitivity (TPR) 95% Confidence Interval AUC = 0.928 (95% CI: 0.901-0.951) R andom Guess Optimal Cutoff (Sens: 0.87, Spec: 0.96) (a) Internal T est 0.0 0.2 0.4 0.6 0.8 1.0 1 - Specificity (FPR) 0.0 0.2 0.4 0.6 0.8 1.0 Sensitivity (TPR) 95% Confidence Interval AUC = 0.858 (95% CI: 0.844-0.872) R andom Guess Optimal Cutoff (Sens: 0.85, Spec: 0.86) (b) T emporal validation 0.0 0.2 0.4 0.6 0.8 1.0 1 - Specificity (FPR) 0.0 0.2 0.4 0.6 0.8 1.0 Sensitivity (TPR) 95% Confidence Interval AUC = 0.808 (95% CI: 0.788-0.826) R andom Guess Optimal Cutoff (Sens: 0.82, Spec: 0.67) (c) Independent e xter nal v alidation Figure 2: ROC curves for model performance e valuation. (a) Inter nal testing ROC cur v e of PKUPH. (b) T emporal v alidation ROC curve of PKUPH. (c) Independent e xternal ROC cur v e of SHTMU . P ocket-K showed stronger discrimination for moderate-to-severe hyper - 128 kalemia 129 Model perf or mance was better f or KDIGO-defined moderate-to-se vere h yperkalemia (serum 130 potassium ≥ 6.0 mmol/L). In the tempor al validation set, the A UROC increased to 0.9399 (95% 131 CI 0.9160–0.9590), with a sensitivity of 89.80% (95% CI 78.24%–95.56%). In the independent 132 e xter nal validation set, the A UR OC was 0.8613 (95% CI 0.8243–0.8940), with a sensitivity of 133 81.52% (95% CI 72.39%–88.13%), as shown in Figure 3. 134 In the independent external set, the negative predictiv e value for moderate-to-se v ere h y- 135 perkalemia was 99.91% (95% CI 99.86%–99.95%), indicating a v ery low probability of missed 136 clinically urgent e v ents in this screening setting. These findings suggest that P ock et-K was more 137 sensitiv e to the more mar ked electroph ysiological abnor malities associated with larger potassium 138 ele v ations. 139 5 0.0 0.2 0.4 0.6 0.8 1.0 1 - Specificity (FPR) 0.0 0.2 0.4 0.6 0.8 1.0 Sensitivity (TPR) 95% Confidence Interval AUC = 0.940 (95% CI: 0.916-0.959) R andom Guess Optimal Cutoff (Sens: 0.90, Spec: 0.96) (a) T emporal Exter nal V alidation 0.0 0.2 0.4 0.6 0.8 1.0 1 - Specificity (FPR) 0.0 0.2 0.4 0.6 0.8 1.0 Sensitivity (TPR) 95% Confidence Interval AUC = 0.861 (95% CI: 0.824-0.894) R andom Guess Optimal Cutoff (Sens: 0.82, Spec: 0.79) (b) Independent External V alidation Figure 3: ROC cur ves f or detection of KDIGO-defined moder ate-to-se vere h yperkalemia (serum potassium ≥ 6.0 mmol/L). (a) T emporal v alidation R OC cur ve in PKUPH. (b) Independent e xter nal v alidation R OC cur v e in SHTMU . P ocket-K captured recognizab le electr ophysiological features of hyper - 140 kalemia 141 T o e xamine the wa v ef or m f eatures underlying model predictions, w e stratified samples into high- 142 risk and low-risk groups according to the predicted probability and compared the signal-av eraged 143 Lead I mor phology between groups. Nor malized hear tbeat segments were extr acted from the 144 ra w signals after temporal alignment and standardization, and group-le v el mean wa v ef or ms 145 with standard deviation bands were then calculated. The clearest diff erences were obser ved 146 in the T -w a ve and QRS regions, consistent with the kno wn electroph ysiological manif estations 147 of h yperkalemia (Figure 4). The low-risk group sho ws a more typical wa v ef or m pattern. These 148 findings suggest that high-risk predictions were driven b y recognizab le wa v ef or m f eatures rather 149 than noise alone. 150 Model-predicted high risk belo w the h yperkalemia threshold ma y serve as 151 a potential marker of greater car diorenal bur den 152 T o better understand model behaviour among samples below the hyperkalemia threshold, we 153 compared the clinical profiles of ref erence-negativ e samples stratified b y model-predicted r isk in 154 the e xter nal v alidation set (Figure 5). Because all samples in this analysis had serum potassium 155 v alues below the diagnostic threshold, the aim w as to deter mine whether model-predicted high 156 risk reflected random error or pref erential identification of a subgroup with greater under lying 157 disease b urden. W e f ound that chronic kidne y disease and hear t f ailure were more common in 158 the model high-r isk group than in the model low-risk group . The prev alence of chronic kidney 159 disease increased from 1.2% in the model low-risk group to 3.2% in the model high-risk group 160 ( P < 0 . 001 ), and the pre v alence of hear t failure increased from 1.3% to 4.4% ( P < 0 . 001 ). These 161 findings suggest that model-predicted high risk below the h yperkalemia threshold was not simply 162 random error . Instead, it may identify a subgroup with greater cardiorenal b urden, e v en when the 163 inde x ed serum potassium value does not e xceed the diagnostic threshold. 164 6 Figure 4: Signal-av eraged wa v ef or m comparison. A ver age Lead I ECG wa vef orms are shown f or patients correctly classified by the model as h yperkalemic (high r isk, red line) and non-hyperkalemic (low risk, blue line). Shaded areas indicate standard deviation. Reference-negative, model low risk Reference-negative, model high risk Comorbidity prevalence among reference-negative samples by model-predicted risk Figure 5: Clinical profiles of reference-negativ e samples stratified b y model-predicted r isk. In the external v alidation set, all samples sho wn had serum potassium values below the diagnostic threshold for hyper- kalemia. They were stratified into a model lo w-risk group and a model high-r isk group according to model output. Chronic kidney disease and hear t f ailure were more common in the model high-risk group . The pre v alence of chronic kidney disease increased from 1.2% in the model lo w-risk group to 3.2% in the model high-risk group ( P < 0 . 001 ), and the pre valence of hear t f ailure increased from 1.3% to 4.4% ( P < 0 . 001 ). 7 P ocket-K trac ked c linically meaningful potassium trajectories o ver time 165 T o illustrate longitudinal trac king at the patient lev el, we selected f our representativ e patients from 166 the validation sets with repeated ECG–potassium measurements ov er time (Figure 6). These 167 patients illustrate se v eral clinically rele v ant longitudinal patter ns, including prog ressive potassium 168 rise, ear ly high-risk detection with subsequent recov er y , recurrent se vere fluctuation, and gr adual 169 biochemical improv ement after treatment. 170 F or P atient A, serum potassium remained below the diagnostic threshold for most of f ollow-up , 171 while the model assigned persistently low r isk. As potassium increased late in f ollow-up and 172 e v entually crossed the h yperkalemia threshold, the predicted risk rose shar ply in parallel. This 173 patter n suggests that the model was sensitive to prog ressive potassium ele v ation and ma y be 174 useful f or identifying impending deterioration bef ore or around threshold crossing. 175 F or P atient B , an ear ly episode of h yperkalemia was observed, during which the predicted risk 176 rose to a high le vel. As serum potassium subsequently declined, model output also decreased 177 and remained low during later f ollo w-up . This patter n suppor ts the ability of the model to detect 178 an acute high-risk state and to retur n to a low-risk range after biochemical recov ery . 179 F or P atient C , potassium fluctuated mar k edly ov er time, including sev ere elev ation, par tial 180 correction, and subsequent recurrence. Model-predicted risk changed in par allel with these 181 biochemical shifts, remaining high during sev ere episodes , decreasing after inter im improv ement, 182 and rising again when potassium rebounded. This patter n suggests that the model ma y capture 183 recurrent disease activity during longitudinal sur veillance . 184 F or P atient D , ser um potassium decreased steadily ov er ser ial measurements, and the 185 predicted risk declined in parallel from an initially high le v el to a substantially lo wer range . This 186 patter n suggests that model output may trac k treatment response or clinical recov er y ov er time in 187 patients with resolving h yperkalemia. 188 P ocket-K supported near-real-time inference in a handheld w orkflo w 189 T o assess potential clinical use in a handheld setting, we implemented a lightweight proof-of- 190 concept version of P ocket-K in a single-lead ECG wor kflow . The prototype device acquired a 191 30-s Lead I recording and transmitted the signal to a paired smar tphone application through 192 Bluetooth Low Energy , where near-real-time inference was perf or med using a connected inf erence 193 pipeline (Figure 7). In representative tests, the system retur ned a predicted r isk of 0.1% f or a 194 nor mokalemic e xample with a ser um potassium concentration of 4.1 mmol/L and 74.5% for a 195 se v ere h yperkalemia e xample with a serum potassium concentration of 6.9 mmol/L within seconds. 196 These results suppor t the technical feasibility of r apid risk estimation in a handheld workflow . 197 DISCUSSION 198 In this multicentre study , a single-lead AI-ECG system initialized from a pretrained f ounda- 199 tion model sho wed clinically useful discrimination f or h yperkalemia in internal testing, temporal 200 v alidation, and independent e xter nal v alidation. Although perf or mance declined as dataset hetero- 201 geneity increased, P ock et-K maintained a high negative predictiv e v alue , suppor ting its potential 202 use as a non-inv asiv e r ule-out screening tool f or people at increased cardiorenal r isk who require 203 repeated potassium sur veillance . We also showed the technical f easibility of near-real-time 204 inf erence in a handheld workflow , providing an initial basis for future prospective deployment 205 studies. 206 Prior studies using 12-lead AI-ECG hav e repor ted strong discrimination f or h yper kalemia and 207 suggest that deep-learning models can detect ECG signatures that are not readily captured b y 208 8 Longitudinal Risk T racking Risk P r obability Serum P otassium Thr eshold (5.5) Patient A Patient B Patient C Patient D Figure 6: Longitudinal trac king of ser um potassium using single-lead AI-ECG. Representative patients showing the model’ s ability to track within-patient potassium changes ov er time. The red line indicates laboratory serum potassium, and the b lue dashed line indicates the model-predicted r isk probability . P atient A shows prog ressive potassium r ise with late threshold crossing. Patient B shows an early h yperkalemic episode f ollowed by sustained reco very . P atient C shows recurrent se v ere fluctuation with corresponding changes in model output. Patient D shows gr adual biochemical impro vement accompanied by declining predicted risk. Overall, these e xamples suggest that model output trac ked clinically meaningful potassium dynamics at the individual-patient le vel. 9 A. Handheld ECG acquisition B. Smartphone-c onnected inference wor kflow 30-s single-lead ( Lead I) ECG recording Pocket-K AI Model Near-real-time inference via smartphone- connected workflow C. Risk outputs Risk alert Figure 7: Proof-of-concept handheld deployment w orkflow of P oc ket-K. (A) A handheld de vice paired with a smar tphone application records a 30-s single-lead (Lead I) ECG. (B) The recorded signal is transmitted to the smar tphone through Bluetooth and processed by a connected inf erence pipeline f or near-real-time risk estimation. (C) Representative outputs from the prototype system show a low predicted h yperkalemia risk for a nor mokalemic example (ser um potassium 4.1 mmol/L) and a high predicted r isk f or a se vere h yperkalemia example (serum potassium 6.9 mmol/L). routine visual inter pretation 22–24 . By contrast, e vidence f or single-lead detection has remained 209 limited to relativ ely small single-centre studies, often without r igorous e xter nal validation or 210 e v aluation across acquisition platf or ms 25–27 . Against this background, our study e xtends the 211 literature b y ev aluating a f oundation-model-based single-lead approach in a larger multicentre 212 setting, with temporal separ ation within one health system and e xternal validation on a diff erent 213 ECG platf or m. The low er discr imination obser v ed in e xter nal v alidation relative to internal testing 214 is therefore not une xpected, but instead reflects a more realistic test of transpor tability f or a 215 signal-limited screening model. 216 These findings also help clarify the most plausib le clinical role of P ock et-K. In lower-pre v alence 217 e xter nal settings, positiv e predictiv e v alue declined whereas negativ e predictiv e value remained 218 high, which is consistent with the e xpected behaviour of a r ule-out screening tool under prev alence 219 shift. This patter n suggests that P oc ket-K is better suited to repeated sur veillance and tr iage 220 than to definitive diagnosis . In practice, such a tool ma y be most useful for identifying low-risk 221 states and f or prompting confir mator y laborator y testing or clinical revie w in patients who require 222 ongoing potassium sur veillance , par ticularly those with advanced chronic kidne y disease, dialysis 223 dependence, or combined cardiac and renal disease . 224 The stronger discrimination obser ved f or moderate-to-se vere h yperkalemia is clinically impor- 225 tant. In our study , this endpoint corresponded to serum potassium ≥ 6.0 mmol/L and theref ore 226 spanned KDIGO-defined moderate and sev ere hyperkalemia. This finding is biologically plau- 227 sible , because larger potassium ele v ations are more likely to produce ov er t repolar ization and 228 conduction abnor malities, increasing signal detectability on ECG. F rom a clinical perspectiv e, 229 improv ed perf ormance in this range is especially relev ant, as the main pr iority of a screening tool 230 in high-risk populations is to minimise missed urgent e vents r ather than to replace biochemical 231 confir mation. 232 The inter pretability and phenotype analyses fur ther suppor t the biological plausibility of the 233 model. Group-le v el wav ef orm differences were concentrated in the T -w a ve and QRS regions, 234 consistent with established electroph ysiological manifestations of h yperkalemia. In addition, 235 among samples below the diagnostic threshold, model-predicted high risk was more common in 236 patients with chronic kidney disease and hear t f ailure. This obser vation raises the possibility that 237 model outputs ma y reflect broader cardiorenal electrophysiological stress r ather than potassium 238 10 concentration alone at a single inde x ed time point. Although this inter pretation remains h ypothesis- 239 generating, it ma y help explain wh y some apparently discordant predictions are not clinically 240 trivial. 241 The longitudinal case analyses and handheld prototype provide complementar y e vidence f or 242 potential clinical translation. Ser ial e xamples suggested that model-predicted r isk changed in 243 parallel with within-patient potassium trajectories, suppor ting the possibility that P oc ket-K ma y 244 capture e v olving potassium-related electroph ysiology o ver time. The proof-of-concept handheld 245 workflow fur ther show ed that near-real-time inference is technically feasib le in a connected 246 smar tphone pathwa y . 247 Our study also pro vides initial e vidence of tr anslational f easibility . A handheld single-lead ECG 248 workflow suppor ted near-real-time inf erence through a connected smar tphone-based pathwa y 249 and ma y allow immediate feedbac k without additional inv asiv e burden. Howe v er , this par t of 250 the study was designed as a proof of concept rather than an e valuation of clinical eff ectiv eness. 251 Prospectiv e studies using nativ e handheld and wear able recordings are theref ore needed to 252 assess usability , signal-quality failure modes , calibration, and the eff ect of AI-guided screening on 253 repeat testing, clinical decision-making, and health-care use. 254 This study has sev eral limitations. First, it used historical routinely collected clinical data 255 and theref ore cannot estab lish whether model-guided screening impro ves clinical outcomes or 256 workflow efficiency . Second, although we included temporal and independent external validation, 257 both health systems were located in China, and broader validation across populations, geogr aphic 258 settings, and device form factors is still needed. Third, the single-lead input was derived from 259 clinical 12-lead ECG systems rather than trained and validated pr imarily on nativ e consumer- 260 de vice recordings. Finally , model perf ormance in the presence of rh ythm abnor malities, motion 261 ar tefact, and low-quality recordings requires more systematic e valuation bef ore large-scale real- 262 world deplo yment. 263 In conclusion, P ock et-K provides multicentre e vidence that a f oundation-model-based single- 264 lead AI-ECG approach can suppor t hyperkalemia screening across temporally separated and 265 e xter nally independent v alidation settings . Its high negativ e predictiv e v alue suggests potential 266 v alue as a scalable r ule-out tool f or frequent potassium sur v eillance in high-risk populations. 267 Prospectiv e studies should now assess how such systems can be integrated into handheld 268 and wearab le care pathwa ys to suppor t earlier detection while preser ving saf ety and clinical 269 inter pretability . 270 METHODS 271 Study design and data sour ces 272 This multicenter observational study used routinely collected de-identified clinical ECG and labo- 273 ratory data and adhered to the TRIPOD+AI repor ting guidelines f or clinical ar tificial intelligence 28 . 274 Data were collected from two geographically independent ter tiar y health systems in China: P eking 275 Univ ersity P eople’ s Hospital (PKUPH, Beijing) and The Second Hospital of Tianjin Medical Univ er- 276 sity (SHTMU , Tianjin). The PKUPH set was e xtracted from the MedEx ECG management system 277 (Jan uar y 2016–Nov ember 2024), while the SHTMU set was retrie ved from the Nalong system 278 (Jan uar y 2024–December 2024). The study w as appro v ed b y the Biomedical Ethics Committee of 279 P eking University (IRB00001052-23152), and the requirement f or inf ormed consent was waiv ed 280 because the analysis used de-identified routinely collected clinical data. 281 11 Study population assemb ly and data partitioning 282 As illustrated in Figure 8, we first screened all patients with a v ailab le ECG data dur ing the study 283 periods. After e xclusion of haemolysed samples, v enous serum potassium measurements were 284 linked to ECG recordings using an ECG-anchored pairing strategy . Specifically , f or each ECG, 285 we searched f or potassium measurements obtained within ± 1 h and retained the closest eligible 286 measurement to f or m a unique ECG–potassium pair . ECGs without any eligible potassium 287 measurement within the predefined time window w ere e xcluded. 288 The PKUPH population was par titioned chronologically at July 2021. Records bef ore this 289 cutoff f ormed the de v elopment set, and records after this cutoff f ormed the temporal v alidation set. 290 T o a void inf or mation leakage, we imposed strict patient-le v el non-ov erlap: any patient appearing 291 in the dev elopment period was excluded entirely from the temporal validation set, ev en if later 292 records were av ailable. Within the PKUPH dev elopment set, unique patients were fur ther divided 293 at the patient le v el into a fine-tune set, a model-selection set, and an inter nal test set in an 8:1:1 294 ratio according to a prespecified protocol. The geographically independent SHTMU dataset w as 295 reser v ed e xclusively f or external validation. 296 Because individual patients could contribute multiple ECG–potassium pairs across time , the 297 number of unique patients ( N ) diff ered from the number of paired records ( n ). 298 Definition of c linical comorbidities 299 Chronic kidney disease and hear t failure w ere defined a prior i using str uctured diagnosis inf or ma- 300 tion recorded on or before the index ECG. In the PKUPH sets, diagnoses were obtained from 301 the hospital diagnosis tab le (field: diagnosis name), and in the SHTMU set, from the structured 302 diagnosis string field ( clinic_diag_str ). Because the original diagnosis entries w ere recorded in 303 Chinese, comorbidities were identified using prespecified rule-based ke yword searches applied to 304 the original diagnosis strings. The English ter ms repor ted below describe the diagnostic concepts 305 used f or classification rather than the literal source strings. 306 Chronic kidney disease w as defined using diagnosis strings corresponding to chronic kidney 307 disease or chronic kidney f ailure in the chronic setting, including chronic kidney disease, chronic 308 renal insufficiency , chronic renal failure , end-stage kidney disease , end-stage renal disease, 309 uraemia, and CKD-equiv alent diagnostic e xpressions. Isolated non-specific ter ms such as renal 310 insufficiency or renal f ailure were not used unless the y were e xplicitly documented as chronic. 311 Hear t f ailure was defined using diagnosis str ings corresponding to hear t failure , including 312 hear t f ailure , congestiv e hear t f ailure , left hear t f ailure, right hear t f ailure, biv entricular hear t f ailure, 313 hear t failure with preserved ejection fr action, and hear t failure with reduced ejection fr action. 314 These comorbidity variables were used for baseline set descr iption and for the analysis of 315 ref erence-negativ e samples stratified b y model-predicted risk in the external validation set. 316 Reference standar d and single-lead signal prepr ocessing 317 V enous ser um potassium ser ved as the ref erence standard. T o improv e ph ysiological correspon- 318 dence between ECG w a vef or ms and laborator y measurements , each ECG was paired with the 319 nearest eligib le potassium result within a ± 1 h windo w after e xclusion of haemolysed samples . 320 This ECG-anchored pair ing strategy was designed to reduce temporal mismatch between the 321 model input and the biochemical ref erence label. 322 Lead I was e xtracted from 12-lead ECG recordings to constr uct a single-lead input. All signals 323 f ollow ed a unified preprocessing pipeline. We applied a 0.5–40 Hz band-pass filter to reduce 324 12 Pek i n g Uni v er s i t y Peo p l e' s Ho s p i tal N = 77,785 Ex c l u ded ( N = 62,322) 29,522 Missing ECG records 32,542 No serum K + test within 1h 258 Poor data quality (hemolysis or low SNR) Pek i n g Uni v er s i t y Peo p l e' s Ho s p i tal N = 15,463 (n = 37,067 pairs) Chronological split into fine-tune and temporal external validation datasets ( Ju l y 2021 ) Dev el o pm en t Co h o r t N = 10,409 (n = 26,145 pairs) Tem p o r al Val i d at i o n Co h o r t N = 5,054 (n = 10,922 pairs) Th e Sec o n d Hos p i t al o f Ti an j i n Med ic al Un i v er s i t y N = 49,415 Ex c l u ded ( N = 30,439) 24,011 Missing ECG records 6,361 No serum K + test within 1h 67 Poor data quality (hemolysis or low SNR) Th e Sec o n d Hos p i t al o f Ti an j i n Med ic al Un i v er s i t y N = 18,976 (n = 25,223 pairs) In d ep en den t Ex t er n al Val i d at io n Dat as et N = 18,976 (n = 25,223 pairs) A. PKUPH site B. TMUSH site Figure 8: ST ARD flowchart for study population selection and multicenter dataset par titioning. P anel A shows set construction at PKUPH, where 77,785 patients were initially screened. A total of 62,322 patients were e xcluded through a multistage quality-control pipeline: 29,522 had no ECG records, 32,542 had no eligible v enous serum potassium measurement within a ± 1-hour window f or ECG-anchored pairing, and 258 were remo ved because of poor data quality , including confirmed laborator y haemolysis or low signal-to-noise ratio . The remaining PKUPH population ( N = 15 , 463 ; n = 37 , 067 pairs) was par titioned chronologically at July 2021 into a dev elopment set ( N = 10 , 409 ; n = 26 , 145 pairs) and a temporal v alidation set ( N = 5 , 054 ; n = 10 , 922 pairs). Panel B shows independent e xternal validation at SHTMU . Of 49,415 initially screened patients , 30,439 w ere e xcluded using the same criter ia (missing ECGs: n = 24 , 011 ; no eligible potassium measurement within ± 1 hour for ECG-anchored pair ing: n = 6 , 361 ; poor data quality: n = 67 ), resulting in a final independent external v alidation set of 18,976 patients with 25,223 ECG– K + pairs. In all panels, N denotes the number of unique patients and n denotes the number of ECG– K + paired records. 13 baseline drift, powerline interf erence, and my oelectric noise, segmented the w av ef orm into non- 325 ov erlapping 10-s clips, and resampled each clip to 500 Hz by linear inter polation to match the 326 input specification of the pretrained f oundation model. Each clip was then z-score normalised to 327 reduce amplitude-scale diff erences across acquisition systems. 328 Model development 329 P ock et-K was de v eloped b y fine-tuning ECGFounder , a pretrained ECG f oundation model. ECG- 330 F ounder adopts a Net1D-style architecture with stage-wise scaling inspired b y RegNet and has 331 been pretrained on more than ten million ECG recordings collected across multiple countr ies 29–31 . 332 This large-scale pretraining enables the model to capture gener al representations of cardiac 333 depolarisation and repolar isation and reduces downstream dependence on sample size and data 334 homogeneity . All fine-tuning experiments were initialised from publicly av ailable ECGFounder 335 pretrained weights . 336 The model was fine-tuned using binar y cross-entropy loss and the Adam optimiser with an 337 initial lear ning rate of 1 × 10 − 4 . T raining was perf or med f or up to 30 epochs. Model selection 338 was based on A UROC in the model-selection dataset. If validation A UR OC did not impro v e f or 339 10 consecutiv e epochs, the lear ning rate was reduced by a factor of 0.1. The checkpoint with 340 the best v alidation A UROC w as retained f or subsequent e v aluation on the internal test dataset, 341 temporal v alidation dataset, and e xternal validation sets. 342 P erf ormance ev aluation and statistical anal yses 343 The primar y endpoint was discrimination for h yper kalemia, defined as v enous serum potassium 344 greater than 5.5 mmol/L. A prespecified secondar y endpoint was discr imination for moderate- 345 to-se v ere h yper kalemia (serum potassium ≥ 6.0 mmol/L). According to the KDIGO 2024 CKD 346 guideline, moderate hyperkalemia is defined as 6.0–6.4 mmol/L and sev ere h yperkalemia as 347 ≥ 6.5 mmol/L 32 . Model discrimination was primarily assessed using the area under the receiv er 348 operating characteristic cur v e (A UROC). 349 Because individual patients could contribute multiple ECG–potassium pairs, statistical un- 350 cer tainty was quantified using clustered bootstrap resampling at the patient lev el with 2000 351 resamples. This framework was used to estimate 95% confidence inter vals for A UROC and 352 threshold-dependent perf or mance metrics and to compare model perf or mance across inter nal 353 test, temporal validation, and e xter nal validation sets without treating repeated paired records 354 from the same patient as independent obser v ations. 355 Additional anal yses and explainability 356 W e perf or med additional analyses to e v aluate clinically rele vant model beha viour be yond binary 357 discrimination. First, moderate-to-se vere h yper kalemia was analysed as a high-prior ity subgroup 358 because of its g reater clinical urgency . Second, wa v ef or m-le v el e xplainability analysis w as per- 359 f or med b y stratifying samples according to model-predicted risk and compar ing signal-av er aged 360 hear tbeat mor phology between high-r isk and low-risk groups, with par ticular attention to re- 361 gions spanning the T w av e and QRS comple x. We also compared clinical phenotypes between 362 f alse-positiv e and true-negative samples in the e xter nal v alidation set to deter mine whether 363 f alse-positiv e predictions were enriched for cardiorenal comorbidity . 364 T o assess whether model outputs trac ked disease dynamics at the individual le v el, we e xam- 365 ined representativ e longitudinal patients with repeated ECG–potassium pairs o v er time. Finally , 366 14 f or proof-of-concept deplo yment, we e v aluated inference latency and qualitativ e risk prompting in 367 a handheld single-lead workflow . 368 Pr oof-of-concept handheld deployment 369 F or proof-of-concept deplo yment, the handheld de vice acquired a 30-s single-lead ECG recording. 370 T o maintain consistency with the temporal scale used during model de velopment, each recording 371 was divided into three consecutiv e 10-s clips f or inf erence. Clip-lev el outputs were then agg re- 372 gated to generate a measurement-lev el risk probability . This design preser ved tempor al-scale 373 consistency between model de v elopment and prototype deplo yment. 374 Dec laration statements 375 Data A vailability 376 The data that suppor t the findings of this study are not publicly av ailable due to restr ictions 377 imposed by institutional ethics committees and data gov ernance policies of the par ticipating 378 hospitals. Access to the data may be considered upon reasonab le request to the corresponding 379 author , subject to approv al by the rele vant ethics committees. 380 Code A vailability 381 The code used f or model de v elopment and e v aluation in this study is publicly a v ailab le at https: 382 //github.com/Tangoz1003/Pocket- K . 383 Ac knowledgements 384 Shenda Hong is suppor ted by the National Natural Science F oundation of China (62102008), 385 CCF-T encent Rhino-Bird Open Research Fund (CCF-T encent RA GR20250108), CCF-Zhipu 386 Large Model Inno vation Fund (CCF-Zhipu202414), PKU-OPPO Fund (BO202301, BO202503), 387 Research Project of P eking University in the State K ey Laborator y of V ascular Homeostasis 388 and Remodeling (2025-SKL VHR-YCTS-02), and the Beijing Municipal Science and T echnology 389 Commission (Z251100000725008). 390 Luxia Zhang is suppor ted b y the National Natur al Science F oundation of China (72125009) 391 and grant from the Noncommunicab le Chronic Diseases-National Science and T echnology Major 392 Project of China (No . 2025ZD0547500). 393 Kangyin Chen is suppor ted by the National Natural Science F oundation of China (82470527) 394 and the K e y Science and T echnology Suppor t Project of Tianjin Science and T echnology Bureau 395 (24ZXGZSY00130). 396 The authors thank all collaborators and par ticipating institutions f or their suppor t and contribu- 397 tions to this research. 398 A uthor Contrib utions 399 Gongzheng T ang, Qinghao Zhao , and Guangkun Nie contributed equally to this work. Gongzheng 400 T ang contributed to methodology dev elopment, model implementation, v alidation, formal analysis, 401 and drafting of the manuscript. Qinghao Zhao contr ibuted to result inter pretation and manuscript 402 re vision. Guangkun Nie contributed to data acquisition, preprocessing, and curation. Y ujie Xiao , 403 15 Shijia Geng, Donglin Xie, Shun Huang, Deyun Zhang, Xingchen Y ao , and Jinwei W ang contributed 404 to data preparation and inv estigation. Kangyin Chen, Luxia Zhang, and Shenda Hong conceiv ed 405 and super vised the study , pro vided resources, guided study design and inter pretation, and revised 406 the manuscript. All authors re view ed and approv ed the final manuscript. Kangyin Chen, Luxia 407 Zhang, and Shenda Hong are corresponding authors and take responsibility f or the integrity of 408 the work. 409 Competing Interests 410 Shenda Hong is an Associate Editor of npj Digital Medicine . Shenda Hong was not in volv ed in 411 the jour nal’ s revie w of, or decisions related to , this manuscr ipt. The other authors declare no 412 competing financial or non-financial interests related to this study . 413 References 414 1. K o vesdy , C.P . (2016). Epidemiology of h yperkalemia: an update. Kidney inter national 415 supplements 6 , 3–6. 416 2. Hougen, I., Leon, S.J ., Whitlock, R., Rigatto , C ., K omenda, P ., Bohm, C ., and T angri, N. (2021). 417 Hyperkalemia and its association with mor tality , cardiov ascular ev ents , hospitalizations, 418 and intensive care unit admissions in a population-based retrospectiv e cohor t. Kidney 419 inter national repor ts 6 , 1309–1316. 420 3. Mclean, A., Nath, M., and Sawhney , S. (2022). P opulation epidemiology of h yperkalemia: 421 cardiac and kidne y long-term health outcomes. American Jour nal of Kidne y Diseases 79 , 422 527–538. 423 4. K o v esdy , C .P ., Matsushita, K., Sang, Y ., Brunskill, N.J ., Carrero , J.J ., Chodic k, G., Hasega wa, 424 T ., Heerspink, H.L., Hiray ama, A., Landman, G.W . et al. (2018). Serum potassium and 425 adv erse outcomes across the r ange of kidne y function: a c kd prognosis consor tium meta- 426 analysis. European hear t jour nal 39 , 1535–1542. 427 5. Go y al, A., Sper tus, J .A., Gosch, K., V enkitachalam, L., Jones, P .G., V an den Berghe, G., and 428 K osiborod, M. (2012). Serum potassium le v els and mor tality in acute m yocardial inf arction. 429 Jama 307 , 157–164. 430 6. Lin, C ., Lin, C .S ., Chen, S.J ., Tsai, S .H., Sung, C .C ., Chen, C .C ., Hsu, Y .J., Hung, Y .J., and 431 Lin, S .H. (2026). Ai-enabled electrocardiog ram aler t f or potassium imbalance treatment: a 432 pragmatic randomiz ed controlled trial. Nature Communications 17 , 159. 433 7. Asir v atham, J .R., Moses, V ., and Bjor nson, L. (2013). Errors in potassium measurement: a 434 laboratory perspective f or the clinician. Nor th Amer ican jour nal of medical sciences 5 , 255. 435 8. Campese, V .M., and Adenuga, G. (2016). Electroph ysiological and clinical consequences of 436 h yperkalemia. Kidney international supplements 6 , 16–19. 437 9. Lin, C ., Chau, T ., Lin, C .S., Shang, H.S ., F ang, W .H., Lee, D .J., Lee , C .C ., Tsai, S.H., W ang, 438 C .H., and Lin, S.H. (2022). P oint-of-care ar tificial intelligence-enabled ecg f or dyskalemia: a 439 retrospectiv e cohor t analysis f or accuracy and outcome prediction. NPJ digital medicine 5 , 8. 440 16 10. Zhao , Q., Geng, S., W ang, B., Sun, Y ., Nie , W ., Bai, B., Y u, C ., Zhang, F ., T ang, G., Zhang, D . 441 et al. (2024). Deep lear ning in hear t sound analysis: from techniques to clinical applications. 442 Health Data Science 4 , 0182. 443 11. Luo , Y ., Liu, X.Y ., Y ang, K., Huang, K., Hong, M., Zhang, J., W u, Y ., and Nie, Z. (2024). 444 T ow ard unified ai drug discov er y with multimodal knowledge . Health Data Science 4 , 0113. 445 12. Zhang, S., Mu, W ., Dong, D ., Wei, J ., F ang, M., Shao , L., Zhou, Y ., He, B., Zhang, S., Liu, 446 Z. et al. (2023). The applications of ar tificial intelligence in digestiv e system neoplasms: a 447 re view . Health Data Science 3 , 0005. 448 13. Liu, X., Gao , K., Liu, B., P an, C ., Liang, K., Y an, L., Ma, J ., He , F ., Zhang, S ., P an, S . et al. 449 (2021). Advances in deep lear ning-based medical image analysis. Health Data Science 450 2021 , 8786793. 451 14. Xiao , Y ., T ang, G., Liu, W ., Li, J., Nie, G., Kan, Z., Zhang, D ., Zhao , Q., and Hong, S. 452 (2025). Any ecg-lab: An e xploration study of fine-tuning an ecg foundation model to estimate 453 laboratory values from single-lead ecg signals. arXiv preprint arXiv:2510.22301. 454 15. Nie, G., Zhu, J ., T ang, G., Zhang, D ., Geng, S ., Zhao , Q., and Hong, S. (2024). A re view of 455 deep lear ning methods f or photopleth ysmogr aph y data. arXiv prepr int arXiv:2401.12783. 456 16. Shi, T ., Ma, J., Y u, Z., Xu, H., Y ang, R., Xiong, M., Xiao , M., Li, Y ., Zhao , H., and K ong, G. 457 (2025). Large language models in critical care medicine: scoping revie w . JMIR Medical 458 Inf or matics 13 , e76326. 459 17. P oter ucha, T .J., Jing, L., Ricar t, R.P ., Adjei-Mosi, M., Finer , J ., Har tzel, D ., K else y , C ., Long, A., 460 Rocha, D ., Ruhl, J.A. et al. (2025). Detecting structural hear t disease from electrocardiograms 461 using ai. Nature 644 , 221–230. 462 18. Rawlani, M., Ieki, H., Binder , C ., Y uan, V ., Chiu, I.M., Bhatt, A., Ebinger , J .E., Sahashi, 463 Y ., Ambrosy , A.P ., Usuku, H. et al. (2025). Ar tificial intelligence prediction of age from 464 echocardiograph y as a mar ker f or cardiov ascular disease. npj Digital Medicine 8 , 688. 465 19. Nie, G., Zhao , Q., T ang, G., Li, Y ., and Hong, S. (2025). Ar tificial intelligence-der iv ed 466 photopleth ysmogr aph y age as a digital biomarker f or cardio vascular health. Communications 467 Medicine 5 , 481. 468 20. Xiao , Y ., T ang, G., Zhang, D ., Li, J ., Nie, G., W ang, H., Huang, S., Liu, T ., Zhao , Q., Chen, 469 K. et al. (2025). Fine-tuning an ecg f oundation model to predict coronar y ct angiograph y 470 outcomes. arXiv preprint arXiv:2512.05136. 471 21. Oikonomou, E.K., V aid, A., Holste, G., Coppi, A., McNamara, R.L., Baloescu, C ., Krumholz, 472 H.M., W ang, Z., Apakama, D .J., Nadkarni, G.N. et al. (2025). Ar tificial intelligence-guided 473 detection of under-recognised cardiomy opathies on point-of-care cardiac ultrasonogr aph y: a 474 multicentre study . The Lancet Digital Health 7 , e113–e123. 475 22. Lin, C .S., Lin, C ., F ang, W .H., Hsu, C .J ., Chen, S.J ., Huang, K.H., Lin, W .S ., Tsai, C .S., K uo , 476 C .C ., Chau, T . et al. (2020). A deep-lear ning algor ithm (ecg12net) for detecting h ypokalemia 477 and h yperkalemia by electrocardiogr aph y: algor ithm de v elopment. JMIR medical informatics 478 8 , e15931. 479 17 23. Har mon, D .M., Heinr ich, C .K., Dillon, J .J ., Car ter , R.E., Kashani, K.B., Attia, Z.I., F r iedman, 480 P .A., and Jentzer , J .C . (2024). Mor tality risk stratification utilizing ar tificial intelligence elec- 481 trocardiogram f or h yperkalemia in cardiac intensiv e care unit patients. JA CC: Adv ances 3 , 482 101169. 483 24. Chen, C .C ., Lin, C., Lee, D .J ., Lin, C .S ., Chen, S.J ., Sung, C .C ., Hsu, Y .J., and Lin, S.H. 484 (2025). Monitoring serum potassium concentration in patients with sev ere h yperkalemia: the 485 role of b loodless ar tificial intelligence-enabled electrocardiogr aph y . Clinical Kidney Journal 486 18 , sf af092. 487 25. Attia, Z.I., DeSimone, C.V ., Dillon, J .J ., Sapir , Y ., Somers, V .K., Dugan, J.L., Bruce, C .J ., 488 Ack erman, M.J., Asir v atham, S.J ., Str iemer , B.L. et al. (2016). No vel bloodless potassium 489 deter mination using a signal-processed single-lead ecg. Jour nal of the Amer ican hear t 490 Association 5 , e002746. 491 26. Ur tnasan, E., Lee , J.H., Moon, B ., Lee, H.Y ., Lee, K., and Y ouk, H. (2022). Noninv asiv e 492 screening tool f or hyperkalemia using a single-lead electrocardiogram and deep lear ning: 493 De v elopment and usability study . JMIR medical informatics 10 , e34724. 494 27. Chiu, I.M., W u, P .J., Zhang, H., Hughes , J .W ., Rogers , A.J ., J alilian, L., P erez, M., Lin, C .H.R., 495 Lee, C .T ., Zou, J . et al. (2024). Serum potassium monitoring using ai-enab led smar twatch 496 electrocardiograms . Clinical Electroph ysiology 10 , 2644–2654. 497 28. Collins, G.S ., Moons , K.G., Dhiman, P ., Rile y , R.D ., Beam, A.L., V an Calster , B ., Ghassemi, 498 M., Liu, X., Reitsma, J .B., V an Smeden, M. et al. (2024). T r ipod+ ai statement: updated 499 guidance f or repor ting clinical prediction models that use regression or machine lear ning 500 methods. bmj 385 . 501 29. Li, J., Aguirre, A.D ., Junior , V .M., Jin, J., Liu, C., Zhong, L., Sun, C., Cliff ord, G., Bran- 502 don W estov er , M., and Hong, S . (2025). An electrocardiog ram f oundation model b uilt on o v er 503 10 million recordings. Nejm ai 2 , AIoa2401033. 504 30. Radosav ovic, I., K osaraju, R.P ., Girshick, R., He, K., and Dollár , P . (2020). Designing netw or k 505 design spaces. In Proceedings of the IEEE/CVF conf erence on computer vision and patter n 506 recognition. pp . 10428–10436. 507 31. Hong, S ., Xu, Y ., Khare, A., Priambada, S., Maher , K., Aljiffr y , A., Sun, J ., and T umanov , A. 508 (2020). Holmes: health online model ensemble ser ving f or deep lear ning models in intensive 509 care units . In Proceedings of the 26th A CM SIGKDD Inter national Conf erence on Kno wledge 510 Discov ery & Data Mining. pp. 1614–1624. 511 32. Le vin, A., Ahmed, S .B., Carrero , J .J ., F oster , B., F rancis , A., Hall, R.K., Herrington, W .G., Hill, 512 G., Ink er , L.A., Kazancıo ˘ glu, R. et al. (2024). Ex ecutiv e summar y of the kdigo 2024 clinical 513 practice guideline for the ev aluation and management of chronic kidne y disease: known 514 knowns and kno wn unknowns . Kidney international 105 , 684–701. 515 18
Original Paper
Loading high-quality paper...
Comments & Academic Discussion
Loading comments...
Leave a Comment