Natural direct effects of vaccines and post-vaccination behaviour
Knowledge of the protection afforded by vaccines might, in some circumstances, modify a vaccinated individual's behaviour, potentially increasing exposure to pathogens and hindering effectiveness. Although vaccine studies typically do not explicitly …
Authors: Bronner P. Gonçalves, Piero L. Olliaro, Sheena G. Sullivan
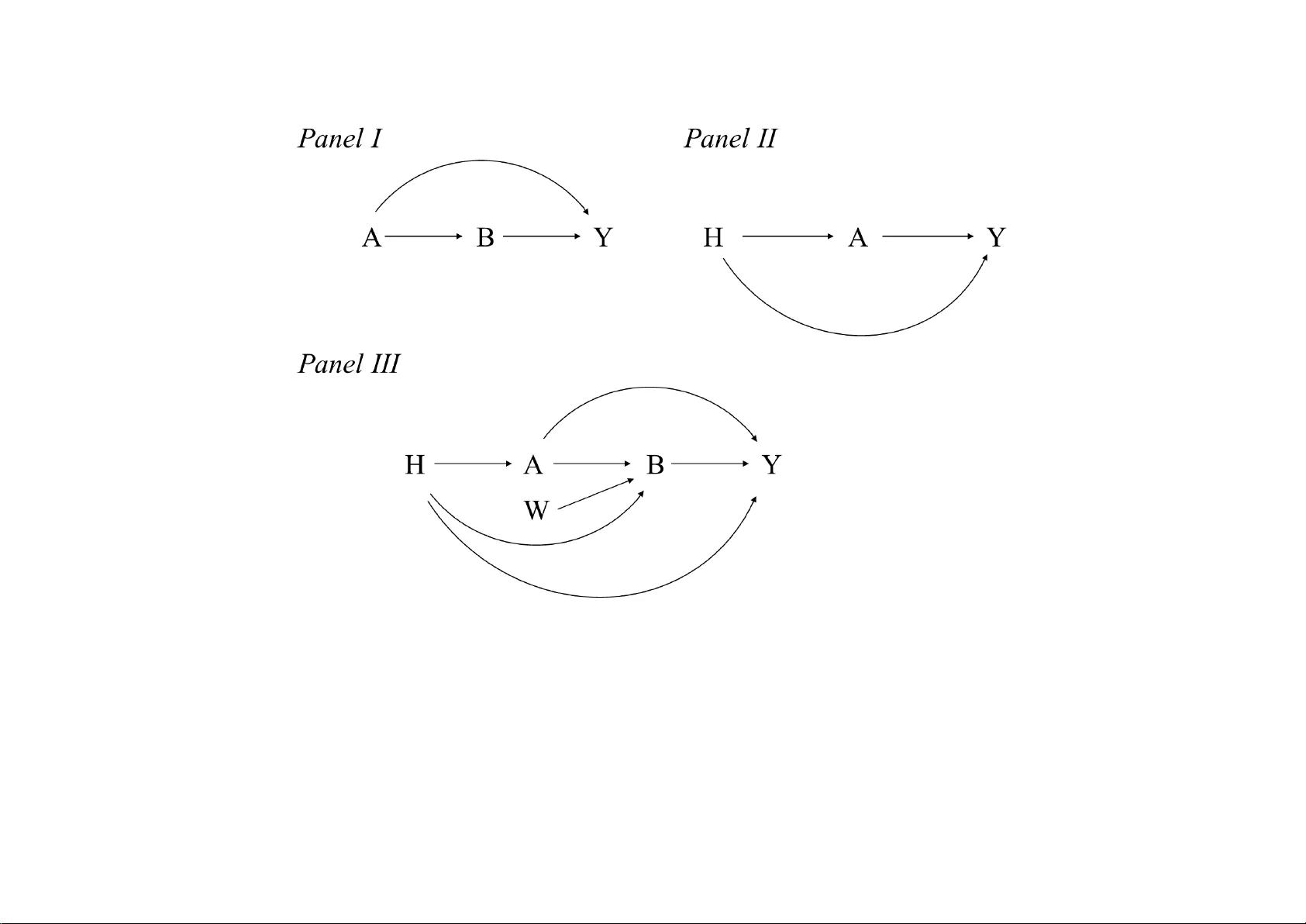
1 T itle Natural direct ef fects of vaccines and post-vaccination behaviour Authors Bronner P . Gonçalves 1,2 , Piero L. Olliaro 2 , Sheena G. Sullivan 3,4 , Benjamin J. Cowling 5 Af filiat ions 1 University of Surrey , Guildford, United Kingdom 2 ISARIC, Pandemic Scienc es Institut e, University of Oxford, Oxford, United Kingdom 3 School of Clinical Science s, Monash Unive rsity , Melbourne VIC, Australia. 4 Fielding School of Public Health, University of California, Los Angeles (U CLA), Los Angeles, California 5 WHO Collaborating Centre for Infectious Disease Epidemiology and Control, School of Public Health, Li Ka Shing Faculty of Medicine, The University of Hong Kong, Hong Kong Special Administrative Region, People's Republic of China Correspondence bronner goncalves@gmail.com , piero.olliaro@ndm.ox.ac.uk , bcowling@hku.hk 2 Abstract Knowledge of the protection af forded by vaccines might, in some cir cumstances, modify a vaccinated individual’ s behaviour , potentially increasing exposure to pathogens and hindering ef fectiveness . Although vaccine studies typically do not explicitly account for thi s possi bility in their analyses, we argue that na tural direct ef f ects might represent a ppropriate causal estimands when an objective is to quantify the ef fect of vaccination on diseas e while “blocking” its influence on behaviour . There are, how ever , complications of a practical nature for the estimation of natural direct effects in this context. Here, w e discuss some of these issues , including exposure-outcome and media tor-outcome confounding by healthcare see kin g behaviour , and possible a pproaches to fa cilit ate estimates of these ef fects. This work highlights the importance of data collection on behaviour , of assessing whether vaccination induces “riskier” behaviour , and of understanding the p otential ef f ects of int erventions on vaccination that could “turn of f” vaccine ’ s influence on behaviour . Keywords causal inference, vaccine ef fectiveness, direct effects, potential outcomes 3 Backgr ound V accination is a preventive intervention whose uptake may be correlated with other health- protective b ehaviou rs . However , vaccination may also le ad to risk compensation, resulting in additional exposures compared to unvaccinated individuals. Hence, the real-world impact of vaccines could be affected by behavioura l changes that occur due to knowledge of the vaccine’ s protective effect. This risk compensation could r esult in a reduced lev el of protection from vaccination in real life compared to what might be expected in a blinded vaccine trial. Specifically , vaccinated individuals might e ngage in activities that increase their risk of infection, either by choice or because of societal or cultural norms, e.g., by incr easing the number of social contacts that c an lead to an infection. Thus, during the COVID-19 pandemic, several studies [1 -4] were performed to assess the influence of vaccinat ion on behaviour associated with infection risk. For exa mple, in France, McColl and colleagues [5] an alysed online surveys on protective behaviours and showed that vaccinated in dividuals were less likely to avoid social gatherings and to wear mas ks in some of the months when surveys were performed. In Canada [6], vaccinated individuals with comorbidities had more social contacts in the third wave of the C OVID-19 pandemic c ompared to unvaccinated individuals with comorbidities. Consistent with this, knowledge a bout vaccination has b een associated with high-risk behaviour [7]. Here, we argue that, al though risk compensation might not be pervasive, effectiveness studies should consider this unintended consequence of vaccination both to quantify an ef fect that is independent of changes in behaviour and to understand potential benefits of interventions that could prevent risk c omp ensation. In particular , we suggest that, along with estimands typically tar geted in vaccine studies, a causal estimand that corresponds to the effect of vaccination in the presence of an intervention that blocks its influence on behaviour might be of value for policy makers, in additio n to being o f sci entific in terest in its own right . Su ch an intervention could, for example, involve encoura ging individuals not to cha nge beha viour afte r vaccination, which might be , in some settings, more re alistic than interventions that a im to set be haviour to a particular level for all individuals in a population. In fact, this latter type of intervention could be conceived of as being related to cont rolled direct effects, whilst the former type of intervention (that does not fix behaviour of all indi viduals to the same level, but ra ther, by 4 blocking the influence of vaccination, allows natural variation in behaviour ) is relevant to natural direct ef fects. Below , to facilitate analyses of direct (with respect to behavioural factors) effects of vaccines on clinical outcomes, we present relevant caus al diagrams, formally define th e proposed effec t , which is, as implied above, a natural direct e f f ect, discuss identification, and compare this effect with that estimated in blinded trials . Further , w e discuss practical issues i n the study of this estimand. For completeness, we also discuss the dist inct question of assessing ef fect s of vaccination on behaviour when information on the latter is not available and the potential impact of interference . Throughout, we focus on observational studies and consider confounding by healthcare seeking behaviour , which might affec t many vaccine effectivene ss analyses. Epidemiologic context and notation Consider a hypothetical study undertaken during an epidemic . Let denote vaccination ( = vaccinated, = not vaccinated), and , the outcome of inter est ( = disease caused by the pathogen targeted by vaccination, = no dise ase caused by the pathogen). In Panel I of Figure 1 , we present the sce nari o described above; corresponds to infection-re late d behaviour (e.g., number of social contacts of a relevant type per time unit) and is assessed after va ccine assignment. W e assume that is a mediator of the effec t of on . Although we consider a scenario where vaccination, on average, leads to “riskier” behaviour among the vaccinated, in some situations, the behavioural ch anges might be linked to absence of vaccination. For example, compliance w ith public health measures during the COVID -19 pandemic was reported, in some coun tries, to be lowest among unvaccinated individuals [8]. Another possibility is for abse nc e of vaccination to re q uire safer b ehaviours. For example, some jurisdictions or healthcare facilities have required healthcare workers who choose not to b e vaccinated against influenza to wear face masks [9, 10]. In observational studies, there might be factors that determine both vaccination and outcome ; we denote common causes of and (that is, con founders) by . One of these common causes is healthcare seeking behaviour; for inst ance, individuals who are more li kely to be vaccinated might also be more likely to go to a clinic or hospital if they become sick. In Panel II of Figu re 5 1 , we illust rate this with variable (healthcare seeking behaviour; note the similarity with Figure 1 in [1 1]). In Panel III o f Figure 1 , we assume that also af f ects . Below , we consider both Panels I and III and a ssum e that information on and (including ) could be collected using, for example, social contact diaries (see [6]) and medical registry databases. W e also define the poten tial outcomes variables and as the values that and would take had been set to . The potential outcomes denote the values would take under interventions on and ; by the composition assumption, . The causal estimand that is relevant in real-world settings ( ) is thus the following: Note that is identified by design in a randomized trial without blinding. As discussed in [12], in trials with blinding, the tar get effect is differe nt (s ee also, below , the section Relation to the e sti mand in vaccine trials ). Finally , notice that in Panel III of Figure 1 , to better e xplain the effect proposed below , we present an other fa ctor affecting , work-related environment ( ). 6 Figure 1 . Causal diagrams representing relations between va ccination, behaviour , and the outcome of interest. In Panel I , we present the causal structure for settings with no confounding; the v ariables are d efined in the main text, and correspond to vaccination ( ), infection-related beh aviour ( ), and clinical disease ( ). In Panel II , to illustrate confounding, the va riable , healthcare seeking b ehaviour , is assumed to a ffec t both and ; we do not present other confounders ( ). In Panel III , we assume that healthcare seeking behaviour affects the exposure ( ), the mediator ( ) and the outcom e ( ); the variable corresponds to work-related environm ent. Although it could be ar g ued that in some settings also directly af fects , here this variable is shown primarily to illustrate causal influences on in the context of natural direc t ef fects (see section Natural dir ect effect of vaccination ). Finally , note that itself might be influenced by risk aversion; however , this is not shown in Figu re 1 as risk a version might af fect variables in the diagram only through its effect on . 7 8 Natural dir ect effect of vaccination Here, w e describe the nat ural direct e f fect ( ) of vaccination relative to . This is the effect of on if we were able to “turn off” the path from to , and is defined as: where is the value that would take had been set to (vaccination) and been set to the value it would take absent vaccination, (which could be different for diffe rent individuals). This estimand [13, 14] corresponds t o the ef fect of on when its ef fect on is blocked, so that the medi ator takes its natural valu e. This could be r epresented in Figure 1 by removing the arrow [15]; in [16], this type of ef fect is re presented by edges crossed out of the graph. Omitti ng th is edge would imply that had no influence on , and would vary based on other possible causes (e.g., would still af fect ). Note that this diffe rs from controlled direct effects as the latter invol ves fixing the value of the mediator for the entire population (i.e., omitting all edges pointing to the mediator). In T able 1 , w e pr esent a numerical example to il lustrate quantitative differences between and . In the example, vaccination increases the probability of risky behaviour , and has a lower absolute value compared to . 9 T able 1. Numerical example. In the table, for si mplicity , we consider binary variables. The variable indicates the event of the number of social contacts being above a pre-defined value , and the outcome, , repre s ents clinical disea se during follow-up. The values for and we r e chosen to illust rate that vaccination can promote risky behaviour. . Note that although and were defined on the risk difference s cale, va ccine studi es typically report effec ti veness, which, numerically , represents the risk difference relative to the risk in the un exposed g roup and here corresponds to and . For the ex ample, the value of would be (in percentage) 32.5% , and that of , 42.5%. 10 Behaviour Proportions 0.70 0.30 0.30 0.70 Clinical outcome Proportions 0.21 0.35 0.14 0.25 Total effect Expected potential outcomes and causal estimand 0.70 x 0.21 + 0.30 x 0.14 = 0.19 0.30 x 0.35 + 0.70 x 0.25 = 0.28 -0.09 NDE Expected potential outcomes and causal estimand 0.30 x 0.21 + 0.70 x 0.14 = 0.16 0.30 x 0.35 + 0.70 x 0.25 = 0.28 -0.12 11 Identification Identification of natural direct effects has been extensively discussed in the causal inference literature [13, 17, 18]. In particular , to identify , standard causal assumptions are not sufficient. When represents the set of common causes of , and (as in Panel III of Figure 1, with re placed by ), the following assumptions allow nonpa rametric identification (below , indicates independence) : 1) 2) 3) 4) In words, within levels of , potential values of Y and of B are independent of vac cination status. Further , the potential value of the out come is independent of behaviour , give n vaccination and . Assumption is a cross-world independe n ce assumption [19, 20], as it involves potential outcome variables under vac cination levels that might not be compatible . In addition to these, positivity assumpti ons such as and for all a, need to hold [21]. For Panel I of Figure 1 , Assumptions , and would hold unconditionally . Under these assumptions, we can identify the : Expr ession 1 The plausibility of these assumptions in observational studies is likely to vary in different contexts. For example, h ealthcare seeking behaviour ( ) is a well-described confounder in studies on total vaccine effects. Addressing confounding by this variable requires quantification 12 of or of proxy variables, and adjustment for healthcare seeking behaviour is often assumed (or not explicitly considered) in ef fectiveness studi es that targe t . In the context of natural direct effects, the li nk might be present, and healthcare seeking behaviour might also correspond to an exposure-mediator a nd mediator -outcome c onfounder . Indeed, while might directly af fect by , for instance, influencing the probability that cases a re medically attended, it is possible that affects , which would imply that could also affec t via . Note that although accounting for healthcare seeking behaviour might be diffic ult , this difficulty is also present in studies on total ef fects. Finally , other factors (e.g., age) may a lso bias a nd , and data on these factors would be required for vaccine mediation analysis. Practical issues While the would provide information that is not obtainable from typical estimands in vaccine studi es, the re are practical iss ues that need to be considered for this type of ef fe ct. First, might be im perfectly measured. In this case, methods have been described for mediation analyses in the pre s ence of misclassific ation [22]. For instance, Ogburn and V anderW eele [23] , in studying non-differential misclassification of a binary mediator , showed that a estimate with this type of measurement error would fall between the true natural direct ef fe ct and the total ef fect (s e e also [24]). Another issue is the possible difficulty in quantifying some aspe cts of b ehaviour linked to infection. For example, McColl and colleagues, in studying protective behaviour and S ARS- CoV -2 vaccination, analysed data on several types of practices that might influence inf ection risk [5]; however , some epidemiologic studies might only be able to capture information on one or two aspects of behaviour . Moreover , the underlying causal structure might be more complex. For inst ance, i n Figure S1 ( Appendix ) , we use two behaviour variables, and ; these varia bles correspond, respectively , to mask use and to number of contacts. In this case, it might still be possible to identify vaccine effects through specific paths (path-specific effe cts [16]); see also work by Zhou and Y amamoto [25] on path-specific effe cts in the presence of multiple, causally-orde re d mediators. In the Appendix , we discuss path-specific effects for Figure S1 . 13 Finally , while capturing information on confounders such as age might be straightforward, accounting for he althcare seeking b ehaviour might require databases with long-term follow-up (with pre-vaccination pe riod) and that are rich enough to include individual-level data on dif ferent aspects of health-related behaviour . There are numerous e xamples of analyses that used data related to healthcare seeking beha viou r during the COVID-19 pandemic [26, 27]. In T able 2 , we c ompare data sources for variables and . 14 T able 2. Data on healthcare se eking behaviour and infection-related behav iour . See also [28], where the authors identified markers for healthcare seeking behaviour in electronic health records, and the work by Bedson and colleagues [2 9] that argues for disease models integrated with behavioural factors. Healthcare seeking behaviour Infection-related behaviour Examples of variables Number of vaccinations targeting another pathogen in the years prior to the study Number of diagnostic tests in the year(s) prior to the study Participation in medical (e.g. cancer) screening activities Factors that might affect healthcare seeking behaviour and that might also be confounders via other paths: age, sex, comorbidities, socioeconomic situation Mask use (Respiratory infections) Number of social contacts (e.g., number of unprotected sexual contacts, for sexually transmitted conditions) Factors that might affect infection- related behaviour and that might also be confounders: age, sex, comorbidities, socioeconomic situation Timing Information collected at baseline (before time zero of follow-up) Data collected after time zero of follow-up and before outcome occurrence Potential data sources Medical registry databases, insurance information Prospective data collection (e.g. social contact diaries, interviews) 15 An alternative causal structur e Above, we assumed that healthcare seeking behaviour is a time-invariant (at least with resp ect to the study ti me scale) characteristic of individuals. In thi s section, we discuss an alternative causal structure in which healthcare seeking behaviour might be af fected by vaccination and thus vary over time. In Figure 2 , variables and correspond to healthcare seeking behaviour before and after vaccine assignment, respectively; in thi s case, the total mediating ef fect through includes the paths and . Here, Assum ption 4 would not hold, as is a c onfounder o f the mediato r-outcome relation affected by . In this situation, although natural direct effe cts would not be nonparametrically identified based on Assumptions 1 – 4, alternative approaches are a vailable: Imai a nd Y amamoto, using linear models, describe sensitivity analyses for this scenario [30]; T chetgen T chetgen and V anderW eele [31] discu ss other identification assumptions; bounds that do not require Assumption 4 could als o be used [19] ; Día z an d Hejazi [32] showed th at direct ef fects fo r stochastic interventions require weaker assumptions ; finally , see work by V anderW eele and colleagues on three meth ods (including one method in which the confounder affected by the exposure and the mediator are considered jointly) [33]. 16 Figure 2. Alternative causal structure representing relations betwee n vaccination ( ), infection-related beh aviour ( ), healthcare seeki ng behaviour ( and ) and clinical outcomes ( ). Here, vaccination af fe cts healthcare seeking behaviour , and thus two variables, for two ti me points (before, , and after , , vaccination), are presented. Note that in some settings, we might want to consider pre -vaccination infection history as a variable that is a parent node of some of t he variables in this diagram, for instance , and , and in this case adjustment for such a variable would be necessary . 17 Relation to the estimand in vaccine trials In a trial with blinding a nd in which the vaccine being tested does not lead to clear side -effects (as the latter would ef f ectively reveal treatment as signment for a fraction of the participants) , vaccination status is not known and hence cannot affect perception of protection . Thus, the estimand in trials might be different from and ; see also [12], where this is discussed under dif ferent causal assumptions . T o define the estimand in blinded trials , we consider an additional v ariable , perception of protection, and assume that the ef fect of on is entirely mediated by ( Figur e S2 ). W e a lso assume: a) that takes values from the set ; b) that in settings without blinding, ; and c) that in bli nded t rials, is set to , which denotes uncertainty about protection . Given this, in a vaccine trial, vaccination ef f ect on ( ) is : where th e second equalit y holds because and the third follows from , as implied by Figure S2 (see for ex ample Section 7.3 in [34]). So, under the causal diagram in Figure S2 , a difference b etween and the other estimands ( and ) is that in a blinded trial, might take a dif ferent value due to uncertainty about vaccine-related protection. Use of alternative outcomes to investigate unascertained vaccine effec ts o n behaviour Many vaccine studies do not collect information on behaviour , which prevents direct assessments of . Here, we consider s cenarios where we might learn about vac cine effects on behaviour despite lack of data on behavioural changes. In Panel I of Figu re 3 , we show a causal structure in which an outcome, , other than the outcome of interest ( ), is presented ; corresponds to infections caused by other pathogens . For instance, could represent COVID-19-related hospi talization and , hospitalization by 18 another respiratory p athogen. W e assume that aspects of beh aviour relevant to are also relevant to , and then ask: When could data on pr ovide information on (if data on ar e not available)? Under causal a ssumpti ons in Panel I of Figure 3 (e.g., absence of cross- reactive immunity ), and after conditioning on , an association between and would indicate that vaccination af fects b ehaviour . In Panel II , some aspects of behaviour are only relevant for the -causing pathogen; here, a vaccine e ffec t on would also suggest risk compensation. In Panel I II , however , some components of behaviour are only relevant for , and thus learning that affe cts does not imply vaccine effects on beh aviour relevant for . Note also that, in Panel I , if affected (e.g., if individuals with the -causing pathogen are [temporarily] resistant to the -causing pathogen), then and would not be d -separated, when controlling for , if the edge was not present, as there would exist the path (further , conditioning on would open the path ). Note that recent work [35] on hidden mediation analysis could be used to quantify direct and indirect ef fects of vaccination with respect to behaviour; in this case, would be a proxy variable of behaviour (see section 3 of [35]); see also [36] on a structurally related que sti on. It is also im portant to mention work on negative control populations [37]; in our context, if, in a subgroup of the population, immune responses are unaffected by vacci nation (e.g. , due to immunosuppression), an association between and in this subgroup would suggest unmeasured confounding or vaccine effects through other paths, including possi bly via behaviour . Finally , and importantly , Stensrud and colleagues [12], in discussing their results, under a dif ferent causal structure, proposed using nega ti ve controls to assess the impact of vaccination on behaviour . 19 Figure 3 . Causal diagrams illustrating vaccine ef f ects in the presence of an alternative infection outcome. In Panels I- III , nodes , , , correspond, respectively , to vac cination, infection- related behaviour , clinical outcome linked to the pathogen of interest, and an alternative infection outcome (caused by another p athogen, not targeted by vaccinati on). In Panel I , denotes healthcare seeking behaviour . In Panels II and III , and repre sent different aspects of beha viour that might af fect and . Note that conf ounders of the relation between and (e.g., ; not shown in the figure) would not imply additional non -causal ope n paths between and , as would be a collider in the path (see, for example, section 5.2 in [38] ). 20 The potential impact of interfer ence In our discussion above, we assume for simplicity no int erfere n ce, i.e., the vaccination status of an individual does not af fect the outcome of other individuals. However , although thi s “no- interference” assumption is often mad e in vaccine studies [39-41], int erference is likely in many studies on infectious diseases. In fact, even for non-communicable conditions , dependence linked to social networks can result in spurious results [42]. In the pr esence of inte rference, potential outcome s are appropriately expr essed using vectors of vaccine assignment to (subgroups of) the population. Using definitions of variables above and assuming that the population is partitioned into subgroups, then potential outcomes of individual in group (w ith and ) cor respond to , where is a vaccine assignment vector in group ; by expressing depe ndence of potenti al outcomes on group-specific assignment, we make a partial interference assumption [43]. When interference is p resent, various effe cts might be defined. For instance, individual total causal e f f ects correspond to , where is the potential outcome of individual in group where individual is assigned a nd assignment to all other individuals in group is re p resented by . Another effect that might be studied under interference is the following direct effec t (“direct” in reference to vaccine assignment of oth er individuals; see section 6 in [43] for dis cussion on direct effect terminology in mediation and interference): . Group- and population-level versions of this ef fect can also be defined [43]. In the context that we conside r in this pape r, the following individual-level effect might be defined: where is the potential outcome of individual in group where individual is assigned vaccination stat us but her behaviour variable takes th e value it would have taken in absence of vaccination, , and assignment for all other individuals in group is repre s ented 21 by . Note that this notation assumes that behaviour is not affec ted by int erference ; howe v er , it is conceivable that it might also depend on the group-level assignment vector , . In observa ti onal studies with interference, identification a nd estimation are, in general, not straightforward. The re have been important developments in this area [43-45], and although beyond the scope of the current wo rk, futu re research on natural direct effe ct s of vaccines could extend this existing li terature, including on causal diagrams fo r interference (see subsection 2.2, which includes discussion on path -specific effects under interference, and sections 3 and 4 in [46]) to clarify identification conditions under interference, or on simulation approaches for network s [47] to assess its potential impact on causal inferences. Note that in contexts with interference, the s eparate question of whether vaccination has spil lover effects (that is, ) is important, and quant ification of this type of effect’ s component that is related to other individuals’ behaviour warrants further investiga ti on in future studies. Discussion Risk compensation migh t affect va c cine ef fectiveness, typically if vaccinees would behave dif ferently from unvaccinated people when social dist ancing and other preventative measures are adopted during epidemi cs, as it has been shown during the COVID -19 pandemic [48, 49]. Thus, it might be particularly important to consider the in these scenarios, even though its identification requires additional assumptions compare d to and to controlled direct ef fects. When estimation of is feasible (i.e., where data on behaviour we re collected and identification assumptions are likely to hold), would provide information on vaccine ef fect if risk compensa ti on could be avoided, hence he lp inform health policy decisions to invest in strategies to minimise the impact of vaccination on behaviour . This paper highlights the implications of post -vaccination infection-related behaviour versus healthcare se eking behaviour when designing empirical studi es and th e need to collect information on behaviour and to investigate vaccine’ s natural direct effects. In trials where blinding prevents participants from knowing vaccination status, vaccine effec t s on behaviour are less li kely – thus the estimated vaccine effect might not correspond to the total effec t in real-world settings , where protection depends on immune responses plus behaviour . A recent study [12] fo rmally described the diffe r ence between the causal effect tar geted in vaccine trials 22 and the effect which operates in communities after vaccine deployment, pro posing definitions of vaccine ef fects account ing for participants’ beliefs on vaccination status. The estimands proposed provide information on both im munologica l and behavioural effects of vaccination by defining interv entions that cor respond to messages with possible v accination status (see expressions 3 and 4 in [1 2] ). The type of ef fect described here is different : we focus on studies that collect b ehavioural information ; a nd we make a distinction between c o ntrolled and na tu ral direct effe cts. W e believe that , in some settings, interventions implied by natural direct ef f ects of vaccines are more plausible than those re lated to controlled direc t effects; note howeve r that we do not claim that the latter type of ef fects is not useful for vaccine-related questions – rather , the relative usefulness of natural versus controlled direct effects might depend on the type of behaviour being considered, which determines the int ervention’ s real-world acceptability . On a related issue, it is possible that participation in trials mi ght be influenced by healthcare seeking behaviour , and that might further affect the e xtern al validity [50] of these studies. W e shoul d mention that alt hough there is evidence for changes in protecti ve behaviour post - vaccination, some studies reported no behavioural changes after vaccination [3, 51] – which could be li nked to cultural factors, or , suggest ef f icient communication by health authorities. W e also know that introducing preventative m easures could have effec ts on behaviour that extend beyond the condition being targeted: for instance, it has been reported that initiation of HIV pre-exposure proph ylaxis might affe ct sexual behaviour [52], exposing to increased risk of sexually transmitted infections. The picture presented here is a simplification of reality , although similar simplifications are often used in epidemiologic studies on vaccines. I ndeed, it is possi ble that future studies might find that the im pact of behavioural changes after vaccination varies consid erably in di fferent settings. Consistent with this, using dynamical modelling of disease transmission, Shaw and Schwartz showed in the context of adaptive netw orks (that is, networks where links between individuals can be “rewired”) that consi derably fewer vaccine resources were needed for epidemic extinction compared to static networks [53]. Moreover , during an epidemic, there might exist temporal trends in protective behaviour , that might follow different patterns for dif ferent types of behaviours [54]; analyses that aim to quantify natural direct ef f ects of vaccines need to account for this. F urther note that while we focused on post -vaccination behaviour , other issues, such as changes in pathogen population composition over time and 23 waning immunity also play a role but are broadly re levant to vaccine studies and were extensively studies for COVID-19 vaccines. Source of f u nding This work was supported by the UK Foreign, Commonwealth and Development Office and W ellcome (215091/Z/18/ Z, 222410/Z/21/Z, 225288/Z/22/Z, and 220757/Z/20/Z); the Bill & Melinda Gates Foundation (OPP1209135); and the philanthropic support o f the donors to t he University of Oxford's COVID-19 R esearch R esponse Fund (0009109). This work was also supported by an RGC Se nior Research Fellowship from the University Grants Commit tee of Hong Kong to BJC (grant number: HKU SRFS2021-7S03). Conflict of inter est statement BJC consults for AstraZeneca, Fosun P harma, GlaxoSmithKline, Haleon, Moderna, Novavax, Pfizer , Roche, and Sanofi Pasteur . All other authors declare no competing interests. 24 Refer ences 1. Bolt, T ., et al., Changes in Behavior After V a ccination and Opinions T owar d Mask W earing: Thoracic Oncology Patient-Reported Experiences During the COVID -19 Pandemic. Clin Med Insights Oncol, 2022. 16 : p. 1 1795549221 123618. 2. Goldszmidt, R ., et al., Pr otective Behaviors Against COVID-19 b y Individual V accination Status in 12 Countries During the Pandemic. JAMA Netw Open, 2021. 4 (10): p. e2131 137. 3. Desrichard, O., L. Moussaoui, and N. Ofosu, R eduction of Pr ecautionary Behaviour following V accination against COVID-19: A T est on a British Cohort . V accines (Basel), 2022. 10 (6). 4. Arashiro, T ., et al., Letter to the editor: Importance of considering high-risk behaviours in COVID-19 vac cin e effectiveness e sti mates with observational studies. Euro Surveill, 2023. 28 (4). 5. McColl, K., et al., Doe s vaccination elicit ris k compensation? Insight s fr om the COVID-19 pande mic in France. Health P sychology and Behavioral Medicine, 2023. 12 (1). 6. Godbout, A., et al., T i me tr ends in social contacts of individuals accor ding to comorbidity and vaccination status, befor e and during the COVID-19 pandemic. BMC Med, 2022. 20 (1): p. 199. 7. T akahashi, S ., et al., A hi gh level of vaccine knowledge incr eases people's behavioral risks for contracting COVID-19 in Japan. Soc Sci Med, 2022. 310 : p. 1 15256. 8. Bodas, M., et al., Lockdown Efficacy in Contr olling the Spr ead of COVID-19 May Be W aning Due to Decline in Public Compliance, Especially among Unvaccinated Individuals: A Cr oss -Sectional Study in Israel. Int J Environ Res Public Health, 2022. 19 (9). 9. Nunn, A., et al., Implementing a pr ovince-wide mandatory vaccinate-or - mask policy at healthcar e facilities in British Columbia, Canada. V accine, 2018. 36 (3): p. 395-399. 10. Rakita, R.M., et al., Mandatory influenza vaccination of healthcar e w orkers: a 5-year study . Infec t C ontrol Hosp Epidemiol, 2010. 31 (9): p. 881-8. 1 1. Lipsitch, M., A. Jha, and L. Simonsen, Observational studies and the diffic ult quest for causality: lessons from vaccine effe ctiveness and impact studies. Int J Epidemiol, 2016. 45 (6): p. 2060-2074. 12. Stensrud, M.J., D. Nevo, and U. Obolski, Distinguishing Immunologic and Behavioral Effects of V accination. Epidemiology , 2024. 35 (2): p. 154-163. 13. Pearl, J., Dir ect and indire ct effects , in Pr oceedings of the S eventeenth confer ence on Uncertainty in artificial intelligence . 2001: Seattle, W ashington. p. 41 1-420 . 14. Robins, J.M. and S. Greenland, Identifiability and ex changeability for dir ect and indir ect effects. Epidemiology , 1992. 3 (2): p. 143-55. 15. Shrier , I. and E. Suzuki, The primary importance of the r esear ch question: implications for understanding natura l versus contr olled dir ect effects. Int J Epidemiol, 2 022. 51 (4): p. 1041-1046. 16. A vin, C., I. Shpitser , and J. Pe arl, Identifiability of path-specific effects , in Pr oceedings of the 19th international joint confer ence on Arti ficial int elligence . 2005: Edinburgh, Scotland. p. 357–363. 17. Hafeman, D.M. and T .J. V ande r W eele, Alternative assumptions for the identification of dir ect and indir ect effects. Epidemiology , 2011. 22 (6): p. 753-64. 25 18. Shpitser , I. and T .J. V anderW eele, A complete graphical criterion for the adjustment formula in mediation analysis. Int J Biostat, 201 1. 7 (1): p. 16. 19. Andrews, R.M. and V . Di delez, Insights into the Cr oss-world Independence Assumption of Causal Mediation Analysis. Epidemiology , 2021. 32 (2): p. 209-219. 20. Naimi, A.I., Invited commentary: boundless science -- putting natural dir ect and indir ect effects in a clear er empirical context. Am J Epidemi ol, 2015. 182 (2): p. 109-14. 21. Nguyen, T .Q., et al., Cl arifying causal mediation analysis: Effect identification via thr ee assumptions and fiv e potential outcomes. J Causal Inf erence, 2022. 10 (1) : p. 246- 279. 22. V anderW eele, T .J., L. V aleri, and E.L. Ogburn, T he r ole of measur ement err or and misclassification in mediation analysis: mediation and measur ement err or . Epidemiology , 2012. 23 (4): p. 561-4. 23. Ogburn, E.L. and T .J. V anderW eele, Analytic r esults on the bias due to nondiffer ential misclassification of a binary mediator . Am J Epid emiol, 2012. 176 (6): p. 555-61. 24. V anderW eele, T .J., et al., Genetic variants on 15q 25.1, smoking, and lung cancer: an assessment of mediation and interaction. Am J Epidemiol, 2012. 175 (10): p. 1013-20. 25. Zhou, X. and T . Y amamoto, T racing Causal Paths fr om Experimental and Observational Data. The Journa l of P olitics, 2023. 85 (1). 26. Dagan, N., et al., Effectiveness of the BNT162b2 mRNA COVID-19 vaccine in pr egnancy . Nat Med, 202 1. 27 (10): p. 1693-1695. 27. Dickerman, B.A., et al., Comparative effectiveness of thir d doses of mRNA-based COVID-19 vaccines in US veterans. Nat Microbiol, 2023. 8 (1): p. 55-63. 28. Graham, S., et al., Identifying markers of health-seeking behaviour and healthcar e access in UK electr onic health r ecor ds. BMJ Open, 2024. 14 (9): p. e081781. 29. Bedson, J., et al., A r eview and agenda for integrated disease models including social and behavioural factors. Nat Hum Behav , 2021. 5 (7): p. 834-846. 30. Imai, K. and T . Y amamoto, Identification and Sensitivity Analysis for Multiple Causal Mechanisms: Revisiting Evidence fr om Framing Expe riments. Politi cal An alysis, 2013. 21 (2): p. 141-171. 31. T chetgen T chetgen, E.J. and T .J. V anderweele, Identification of natural dir ect effects when a confounder of the mediator is dir ectly affected by exposur e. Epidemiology , 2014. 25 (2): p. 282-91. 32. Díaz, I. a nd N.S. Hejazi, Causal Mediation Analysis for Stochastic Interventions. Journal of the Royal Statistical Society Series B: S tatistical Methodology , 2020. 82 : p. 661-683. 33. V anderweele, T .J., S. V ansteelandt, and J.M. Robins, Effect dec o mposition in the pr esence of an exposur e-induced mediator-outcome confounder . Epidemiology , 2014. 25 (2): p. 300-6. 34. Pearl, J., C ausality: Models, Reasoning, and Infer ence . 2nd Edition ed. 2009: Cambridge University Press. 35. Ghassami, A., et al., C ausal infer ence with hidden mediators. Biometrika, 2025. 1 12 (1): p. asae037. 36. Liu, K., R. Altman, and V . Syrgkanis, Detecting clinician implicit biases in diagnoses using pr oximal causal infer ence. Pac Symp Biocomput, 2025. 30 : p. 330-345. 37. Piccininni, M. and M.J. Stensrud, Using Negative Contr ol Populations to Asse ss Unmeasur ed Confounding and Dir ect Effects. Epidemiology , 2024. 35 (3): p. 313-319. 38. Pearl, J., Causal Diagrams for Empirical Resear ch. Biometrika, 1995. 82 (4): p. 669– 688. 26 39. Hernández-Díaz, S., et al., Emulating a T ar get T rial of Interventions Initiated During Pr egnancy with Healthcar e Databases: The E xample of COVID -19 V accination. Epidemiology , 2023. 34 (2): p. 238-246. 40. Ciocănea-T eodorescu, I., et al., Adjustment for Disease Severity in the T e st-Negative Study Design. Am J Epidemiol, 2021. 190 (9): p. 1882-1889. 41. Ortiz-Brizuela, E., et al., Potential biases in test -negative design studi es of COVID-19 vaccine effectiveness arising fr om the inclusion of asymptomatic individuals. Am J Epidemiol, 2025. 194 (3): p. 844-856. 42. Lee, Y . and E.L. Ogburn, Network Dependence Can Lead to Spurious Associations and Invalid Infer ence. Journal of the American S tatistical Association, 2021. 1 16 (535): p. 1060–1074. 43. T chetgen T chetgen, E.J. and T .J. V anderW eele, On causal infer ence in the pr esence of interfer ence. Stat Methods Med Res, 2012. 21 (1): p. 55-75. 44. Hudgens, M.G. and M.E. Halloran, T owar d Causal Infer ence W ith Interfer ence. J Am Stat Assoc, 2008. 103 (482): p. 832-842. 45. Sävje, F ., P . Aronow , and M. Hudgens, A VERAGE TREA TMENT EFFECTS IN T HE PRESENCE OF UNKNOWN INTERFERENCE. Ann Stat, 2021. 49 (2): p. 673-701. 46. Ogburn, E.L. and T .J. V anderW eele, Causal Diagrams for Interfer ence. Statistical Science, 2014. 29 (4): p. 559-578. 47. Zivich, P .N., et al., Ass ortativity and Bias in Epidemiologic Studies of Contagi ous Outcomes: A Simulated Example in the Context of V accination. Am J Epidemiol, 2021. 190 (1 1): p. 2442-2452. 48. Dye, C. and M.C. Mills, COVID-19 vaccination passports. Science, 2021. 371 (6535): p. 1 184. 49. Dada, S., et a l., Learning fr om the past and pre sent: social science impli cations for COVID-19 immunity-based documentation. Humanities and Social Sciences Communications, 2021. 8 (219). 50. Degtiar , I. and S. Rose, A Review of Gen eralizability and T ransportability . Annual Review of Statistics and Its Application 2023. 10 : p. 501-524. 51. Chen, F ., et al., Inve sti gating the causal effects of COVID-19 vac cina tion on the adoption of pr otective behaviors in Japan: Insights fr om a fuzz y r egr ession discontinuity design. PLoS One, 2024. 19 (6): p. e0305043. 52. Oldenbur g, C.E., et al., Behavioral Changes Following Uptake of HIV Pre-exposur e Pr ophylaxis Among Men Who Have Sex with Men in a Clinical Setting. AIDS Behav , 2018. 22 (4): p. 1075-1079. 53. Shaw , L.B. and I.B. Schwartz, Enhanced vaccine contr ol of epidemics in adaptive networks. Phys Rev E Stat Nonlin Soft Matter Phys, 2010. 81 (4 Pt 2): p. 046120. 54. Petherick, A., et al., A worldw ide assessment of changes in adhe r ence to COVID -19 pr otective behaviours an d hypothesized pandemic fatigue. Nat Hum Behav , 2021. 5 (9): p. 1 145-1 160. 27 Appendix T able of contents Path-specific effects and infection-r elated behaviour Figur e S1 Figur e S2 Refer ence 28 Path-specific effects and infection-r elated behaviour Here, we briefly discuss Figure S1 , where two dif ferent aspects of behaviour are present ed: corresponds to mask use, and , to number of social contacts. In this setting, we might be interested in the e f f ect of vaccination on the outcome if its effect on mas k use, but not that on social contacts, were “turned of f”. This could be defined as: Similarly , the effe ct of v accination on the clinical outcome if we were able to block its effe ct on the number of social contacts would be: Further , based on Figure S1 , the total ef fect can be decomposed (see also [1] ): where the first two average contrasts correspond t o mediated effe cts and th e third, to a direct ef fect. 29 Figure S1. C ausal structure including two aspects of behaviour potentially af fected by vaccination. corresponds to mask use, and , to number of social c ont acts. 30 Figure S2. Causal diagram similar to Panel I of Figure 1 and that also includes the variable , which denotes perception of vaccine -related protection. Note that the causal assumptions implied by this directed acyclic graph include: affects only through ; af fects only through . 31 Refer ence 1. Imai, K. and T . Y amamoto, Identification and Sensitivity Analysis for Multiple Causal Mechanisms: Revisiting Evidence fr om Framing Expe riments. Politi cal An alysis, 2013. 21 (2): p. 141-171.
Original Paper
Loading high-quality paper...
Comments & Academic Discussion
Loading comments...
Leave a Comment