ReactEMG Stroke: Healthy-to-Stroke Few-shot Adaptation for sEMG-Based Intent Detection
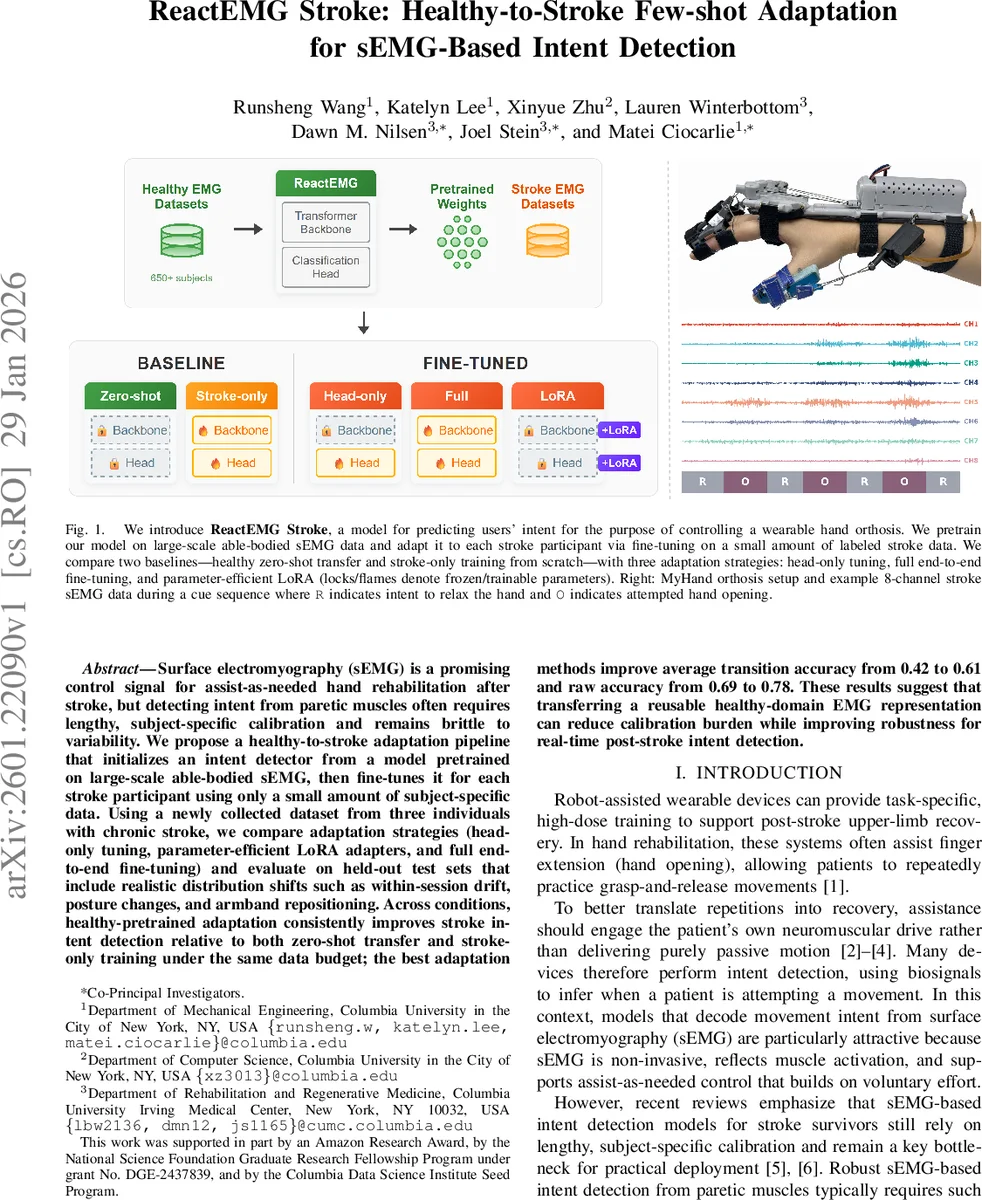
Surface electromyography (sEMG) is a promising control signal for assist-as-needed hand rehabilitation after stroke, but detecting intent from paretic muscles often requires lengthy, subject-specific calibration and remains brittle to variability. We propose a healthy-to-stroke adaptation pipeline that initializes an intent detector from a model pretrained on large-scale able-bodied sEMG, then fine-tunes it for each stroke participant using only a small amount of subject-specific data. Using a newly collected dataset from three individuals with chronic stroke, we compare adaptation strategies (head-only tuning, parameter-efficient LoRA adapters, and full end-to-end fine-tuning) and evaluate on held-out test sets that include realistic distribution shifts such as within-session drift, posture changes, and armband repositioning. Across conditions, healthy-pretrained adaptation consistently improves stroke intent detection relative to both zero-shot transfer and stroke-only training under the same data budget; the best adaptation methods improve average transition accuracy from 0.42 to 0.61 and raw accuracy from 0.69 to 0.78. These results suggest that transferring a reusable healthy-domain EMG representation can reduce calibration burden while improving robustness for real-time post-stroke intent detection.
💡 Research Summary
This paper addresses a critical bottleneck in EMG‑based intent detection for post‑stroke hand rehabilitation: the need for lengthy, subject‑specific calibration due to the substantial differences between paretic and healthy muscle signals. The authors propose “ReactEMG Stroke,” a transfer‑learning framework that leverages a large‑scale, healthy‑domain foundation model (ReactEMG) and adapts it to individual stroke participants using only a few labeled EMG trials.
ReactEMG is an encoder‑only transformer pretrained on five public datasets comprising over 650 able‑bodied participants. It learns a multimodal masked‑modeling objective that jointly reconstructs EMG and intent labels, thereby capturing robust spatiotemporal patterns in healthy sEMG. In the proposed pipeline, this pretrained backbone is fine‑tuned for each stroke participant with a limited dataset (1, 4, or 8 pairs of open/close attempts). Three adaptation strategies are evaluated: (1) head‑only tuning (only the classification head is updated), (2) LoRA (low‑rank adapters added to every linear layer, keeping the original weights frozen), and (3) full‑model fine‑tuning (all parameters are updated). Two baselines are also considered: healthy zero‑shot (no adaptation) and stroke‑only training from scratch.
Data were collected from three chronic‑stroke individuals using an 8‑channel Myo armband (200 Hz) while they attempted hand opening and closing with a MyHand orthosis. Each participant contributed four training sets (standard seated posture) and five test sets designed to simulate realistic distribution shifts: within‑session drift (mid‑session and end‑session), an unseen hovering posture, a 15° counter‑clockwise armband rotation, and a device‑driven closing sequence.
Model selection employed a 4‑fold cross‑validation over the training sets to choose learning rate, regularization, and epoch count. For data‑efficiency experiments, the authors sampled N ∈ {1, 4, 8} pairs from the 12 available training pairs, repeated the process 12 times per N, and reported mean performance. Convergence was examined by training each variant for 100 epochs and evaluating checkpoints every 5 epochs on both the stroke test sets and a held‑out healthy subject from the ROAM‑EMG dataset.
Two metrics capture performance: (i) raw accuracy (frame‑wise label match) and (ii) transition accuracy (the ReactEMG‑specific measure that rewards correct detection of intent transitions within a short reaction window and penalizes flicker during sustained intent). Transition accuracy is particularly relevant for real‑time control because it reflects delayed switching and brief misclassifications that can destabilize a robotic orthosis.
Results show that healthy‑pretrained adaptation consistently outperforms both zero‑shot transfer and stroke‑only training across all test conditions. Full‑model fine‑tuning achieves the highest average transition accuracy (0.61) and raw accuracy (0.78). Head‑only tuning and LoRA also improve performance, reaching transition accuracies of 0.55 and 0.58, respectively, and raw accuracies of 0.73 and 0.75. Importantly, even with only four training pairs (≈8 trials), the adapted models surpass stroke‑only baselines by 10–15 percentage points, and with a single pair they still gain at least 5 % absolute accuracy. Convergence curves reveal rapid gains within the first 20–30 epochs, after which performance plateaus or slightly declines, indicating that few‑shot adaptation can be achieved quickly without extensive training.
The study demonstrates that a foundation model trained on abundant healthy EMG data captures generic muscle activation structures that remain useful for the altered, noisy signals of stroke patients. By fine‑tuning this representation, the system reduces calibration time dramatically while delivering robust performance under realistic variations in posture, sensor placement, and fatigue‑induced drift.
Future directions include expanding the gesture vocabulary, integrating additional modalities (e.g., inertial sensors), exploring meta‑learning or continual‑learning schemes for lifelong adaptation, and deploying the framework in larger clinical trials. Nonetheless, the current work establishes a practical, data‑efficient pathway for bringing EMG‑driven assist‑as‑needed hand orthoses into real‑world stroke rehabilitation.
Comments & Academic Discussion
Loading comments...
Leave a Comment