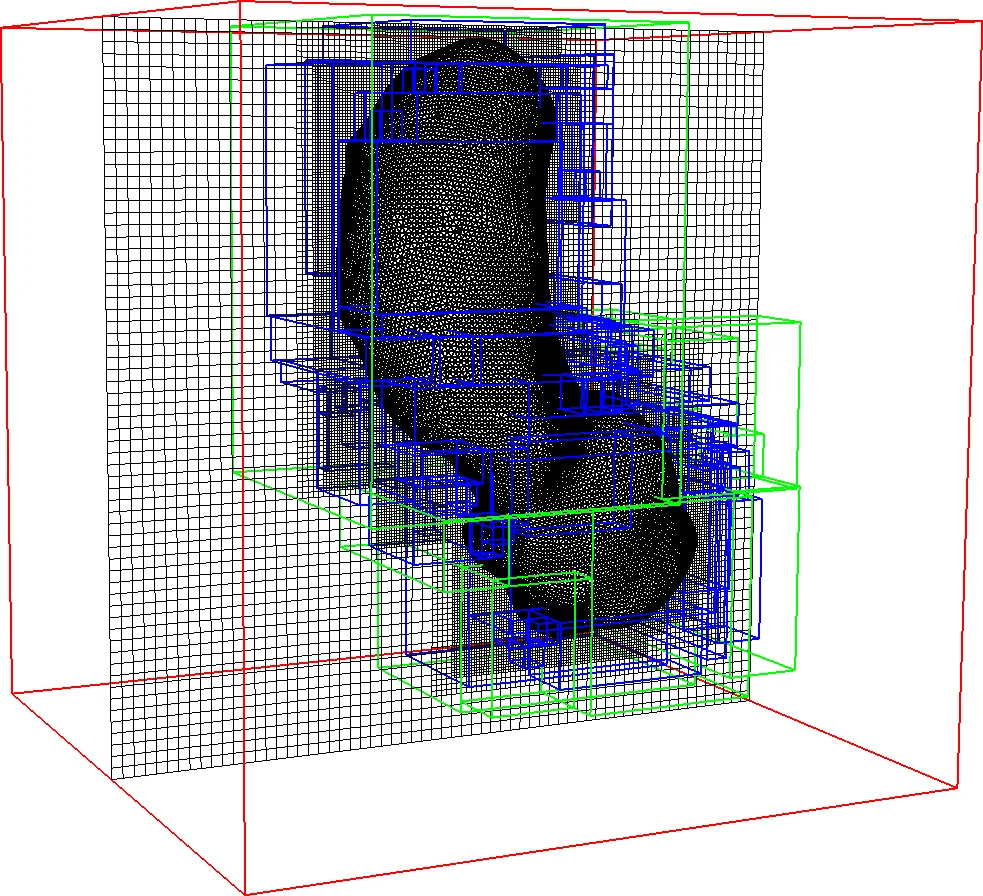
Image-based immersed boundary model of the aortic root
Each year, approximately 300,000 heart valve repair or replacement procedures are performed worldwide, including approximately 70,000 aortic valve replacement surgeries in the United States alone. This paper describes progress in constructing anatomically and physiologically realistic immersed boundary (IB) models of the dynamics of the aortic root and ascending aorta. This work builds on earlier IB models of fluid-structure interaction (FSI) in the aortic root, which previously achieved realistic hemodynamics over multiple cardiac cycles, but which also were limited to simplified aortic geometries and idealized descriptions of the biomechanics of the aortic valve cusps. By contrast, the model described herein uses an anatomical geometry reconstructed from patient-specific computed tomography angiography (CTA) data, and employs a description of the elasticity of the aortic valve leaflets based on a fiber-reinforced constitutive model fit to experimental tensile test data. Numerical tests show that the model is able to resolve the leaflet biomechanics in diastole and early systole at practical grid spacings. The model is also used to examine differences in the mechanics and fluid dynamics yielded by fresh valve leaflets and glutaraldehyde-fixed leaflets similar to those used in bioprosthetic heart valves. Although there are large differences in the leaflet deformations during diastole, the differences in the open configurations of the valve models are relatively small, and nearly identical hemodynamics are obtained in all cases considered.
💡 Research Summary
This paper presents a patient‑specific, image‑based immersed boundary (IB) framework for simulating the fluid‑structure interaction (FSI) of the aortic root and ascending aorta. Starting from a publicly available computed tomography angiography (CTA) dataset, the authors segment the aortic root and ascending aorta using ITK‑SNAP’s active‑contour method, then manually adjust idealized valve leaflet geometries to fit the patient anatomy. Because CTA does not reveal collagen fiber orientation, a rule‑based Poisson interpolation is employed: two Laplace equations with distinct boundary conditions generate scalar fields u and v, whose gradients define a local orthogonal material basis (v₁ = ∇u × ∇v, v₃ = ∇v, v₂ = v₃ × v₁). This basis captures the commissure‑to‑commissure fiber direction and the through‑leaflet normal.
The mechanical response of the leaflets is modeled with a fiber‑reinforced hyperelastic constitutive law. Parameters are calibrated against tensile tests on fresh porcine leaflets and on glutaraldehyde‑fixed leaflets (representative of bioprosthetic valves). The solid mechanics are expressed in a finite‑strain continuum formulation (deformation gradient F, Piola‑Kirchhoff stress Pₛ) and coupled to an incompressible Newtonian fluid (ρ, μ) on a fixed Eulerian grid via the IB delta‑function. The resulting equations enforce a single continuous velocity field u across fluid and solid, automatically preventing interpenetration and handling leaflet‑leaflet contact during diastole.
Temporal integration uses a second‑order predictor‑corrector scheme; spatial discretization employs practical grid spacings of 0.5–0.75 mm, sufficient to resolve leaflet deformation in both diastole and early systole. Inflow and outflow are coupled to a three‑element Windkessel model to reproduce realistic pressure waveforms, and the computational domain is truncated upstream at the left ventricular outflow tract and downstream before the first aortic branch.
Simulation results show that fresh leaflets undergo larger diastolic deformation and achieve a tighter seal under physiological diastolic pressure, whereas glutaraldehyde‑fixed leaflets are stiffer and deform less. Despite these differences, systolic opening configurations, flow rates, stroke volume, and vortex structures are nearly identical (differences < 5 %). The model reproduces physiological cardiac output and maintains convergence over multiple cardiac cycles. Comparison with 4‑D MRI data confirms that the overall flow patterns are realistic.
The study demonstrates that integrating patient‑specific geometry, rule‑based fiber architecture, and experimentally calibrated hyperelastic material models within an IB‑FSI framework yields a robust, clinically relevant simulation tool. It overcomes previous limitations related to mesh generation, contact handling, and simplified leaflet mechanics, and it is readily extensible to evaluate transcatheter aortic valve replacement (TAVR) devices, predict paravalvular leak, or support personalized treatment planning. Future work will expand the cohort size, incorporate non‑Newtonian blood rheology, and couple the model with device‑specific stent structures to further enhance its translational impact.
Comments & Academic Discussion
Loading comments...
Leave a Comment