Biomechanical conditions of walking
The development of rehabilitation training program for lower limb injury does not usually include gait pattern design. This paper introduced a gait pattern design by using equations (conditions of walking). Following the requirements of reducing force to the injured side to avoid further injury, we developed a lower limb gait pattern to shorten the stride length so as to reduce walking speed, to delay the stance phase of the uninjured side and to reduce step length of the uninjured side. This gait pattern was then verified by the practice of a rehabilitation training of an Achilles tendon rupture patient, whose two-year rehabilitation training (with 24 tests) has proven that this pattern worked as intended. This indicates that rehabilitation training program for lower limb injury can rest on biomechanical conditions of walking based on experimental evidence.
💡 Research Summary
The paper presents a biomechanical framework for designing gait patterns specifically aimed at early rehabilitation of unilateral lower‑limb injuries. Recognizing that conventional rehabilitation programs rarely incorporate gait‑pattern design, the authors formulate four fundamental equations (1‑4) that relate vertical ground reaction force (VGRF), stride timing, stride length, and walking speed. Equation 1 enforces that the integral of the VGRFs of the injured and uninjured sides over a stride must equal the body weight, implying that the injured side’s peak VGRF can be reduced either by increasing the uninjured side’s VGRF or by delaying the uninjured side’s stance phase. Equation 2 describes the temporal relationships among double‑support, single‑support, and swing phases, showing that extending the double‑support intervals of the uninjured limb while shortening its single‑support interval lengthens the overall stance of the uninjured side and reduces load on the injured side. Equation 3 links stride length to the individual step lengths of each limb, indicating that shortening the step length of the uninjured side (or equivalently increasing the step length of the injured side) reduces overall stride length. Equation 4 connects walking speed, cadence, and stride length, emphasizing that speed reduction is most efficiently achieved by decreasing stride length rather than altering cadence.
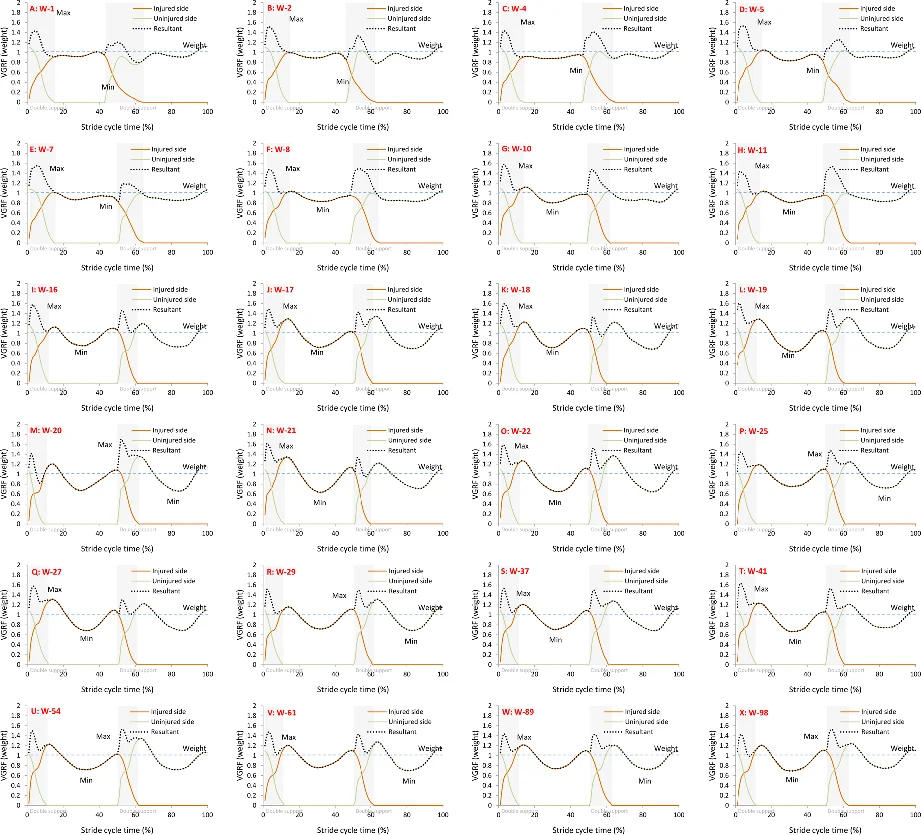
From these equations the authors derive three concrete design principles for a protective gait: (1) delay the stance phase of the uninjured limb, (2) reduce the step length of the uninjured limb, and (3) lower walking speed by shortening stride length. To test the hypothesis, a single 50‑year‑old male patient with an acute Achilles tendon rupture (ATR) was recruited. After surgical repair and cast removal, the patient began gait training using a walking stick while following the proposed gait pattern. Over a two‑year period, 24 gait analyses were performed using a ZEBRIS force‑plate system, capturing step length, stance/swing durations, double‑support time, cadence, speed, and normalized VGRF for each limb.
The results confirmed the theoretical predictions. The uninjured side’s stance phase was indeed delayed, and its step length was reduced, leading to a noticeable decrease in the injured side’s peak VGRF, which approached the subject’s body weight. Stride length and walking speed were both reduced in line with Equations 2–4, while the double‑support and single‑support times of the uninjured side were significantly longer than those of the injured side (p < 0.01). Statistical analysis demonstrated that the gait parameters changed consistently across the 24 testing weeks, supporting the robustness of the design.
The study’s strengths lie in its explicit mathematical modeling of gait biomechanics, the clear translation of those models into actionable training cues, and the empirical verification with a real patient over an extended rehabilitation timeline. However, the work is limited by its single‑case design, lack of a control group, and focus on short‑term biomechanical outcomes without assessing longer‑term functional recovery (e.g., muscle strength, balance, gait symmetry). Moreover, the paper does not provide a detailed protocol for delivering real‑time feedback or for integrating assistive devices that could enforce the prescribed timing adjustments in a clinical setting.
In conclusion, the authors demonstrate that by manipulating stride length, cadence, and especially the timing of the uninjured limb’s stance phase, clinicians can effectively reduce the load on an injured lower‑limb during early gait training. The four‑equation framework offers a theoretically sound and experimentally validated basis for designing protective gait patterns, and it could serve as a foundation for future multi‑subject studies, development of feedback‑driven gait training systems, and broader rehabilitation guidelines for unilateral lower‑limb injuries.
Comments & Academic Discussion
Loading comments...
Leave a Comment