Easy steps towards a sane IT policy in hospitals
We witnessed the low quality of IT solutions in Paris hospitals. The price paid to private companies for these solutions and the cost incurred from their inefficiency constitute a gross and appalling waste of public resources. We propose to bootstrap a change in IT policy by having heads of department hire IT workers ; we give advice to the central decision making body on how to incentivize them. Easily measurable efficiency gains as well as hard-to-quantify positive externalities will follow.
💡 Research Summary
**
The paper “Easy steps towards a sane IT policy in hospitals” by Edouard Klein (2018) documents the chronic inefficiencies of the electronic medical record (EMR) system used in Paris public hospitals, specifically the Cristal‑Net platform. Cristal‑Net, originally released in 2001, still runs only on Windows XP with Internet Explorer 6, making it slow, crash‑prone, and difficult to maintain. The author highlights two intertwined problems: (1) the routine, error‑prone data‑entry task required to extract clinical data for research is delegated to medical residents, diverting them from patient care, teaching, and research; (2) residents lack IT skills, leading to mistakes, data loss, and compromised patient confidentiality.
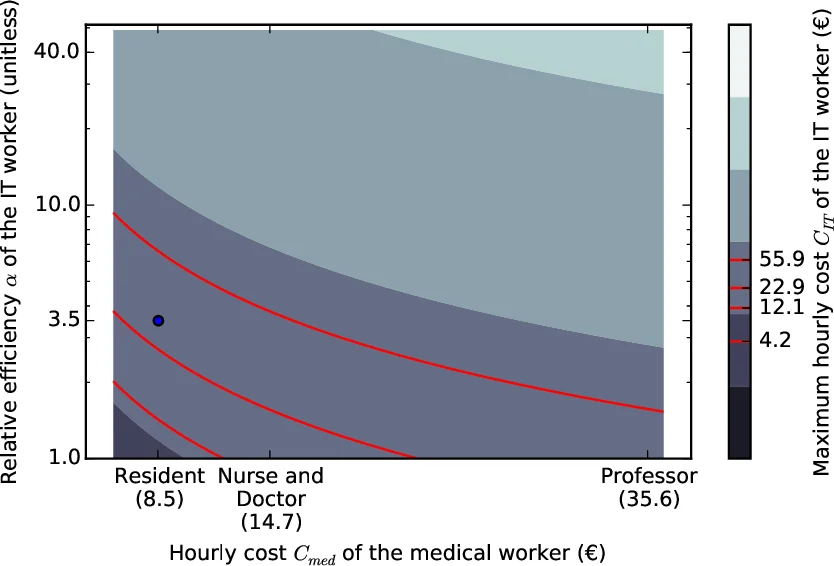
To address these issues, the author proposes a two‑fold solution. The first component is a lightweight automation tool that mimics mouse clicks and keyboard strokes, reads screen images, and navigates Cristal‑Net automatically. In a pilot study, the tool extracted data from over 1,100 records that would have required 41 hours of manual work in only 2 hours of automated execution, after 11 hours of development and testing. This yields an efficiency factor α = t_med / t_IT ≈ 3.5, meaning one hour of IT work saves 3.5 resident‑hours.
The second component is a policy recommendation: each clinical department should directly hire its own IT specialist (or at least an intern) rather than relying on a central IT department that focuses on maintenance rather than development. A simple cost‑benefit model is presented: the gain G = cost(med) − cost(IT) = t_med·C_med − t_IT·C_IT. Hiring an IT worker is advantageous when C_IT ≤ α·C_med. Using realistic hourly costs (resident ≈ 8.5 €/h, nurse/doctor ≈ 14.7 €/h, professor ≈ 35.6 €/h) and α = 3.5, the model shows that an IT worker paid up to about 22.9 €/h still yields net savings. The author further argues that as the IT worker becomes embedded, α will increase (potentially to 10 or even 40) because reusable code libraries, domain knowledge, and process improvements accumulate, creating a compounding benefit.
Policy advice includes designing incentives that reward performance, research output, and skill development while avoiding perverse incentives such as rigid quantitative targets that could undermine quality. The paper stresses that effective EMR solutions will emerge from bottom‑up collaboration between clinicians and IT professionals, not from top‑down mandates.
Related work is surveyed, noting that many hospitals worldwide suffer from similar legacy systems and that open‑source, agile development practices can mitigate these problems. The conclusion reiterates that a modest investment in department‑level IT staffing, coupled with simple automation tools, can free resident time, improve data quality, accelerate research, and ultimately save public funds. However, the author acknowledges that implementation will require navigating hospital governance, labor unions, and budgeting processes, and calls for further field trials to refine the proposed model.
Comments & Academic Discussion
Loading comments...
Leave a Comment